Article Text

Abstract
In Asia Pacific, most countries have expanded HIV treatment guidelines to include all those with HIV infection and adopted antiretroviral treatment for prevention (TFP) as a blanket strategy for HIV control. Although the overall epidemic development associated with this focus is positive, the HIV epidemic in men who have sex with men (MSM) is continuing unperturbed without any signs of decline or reversal. This raises doubt about whether TFP as a blanket HIV prevention policy is the right approach. This paper reviews currently available biomedical HIV prevention strategies, national HIV prevention policies and guidelines from selected countries and published data on the HIV cascade in MSM. No evidence for efficacy of TFP in protecting MSM from HIV infection was found. The rationale for this approach is based on assumptions about biological plausibility and external validity of latency-based efficacy found in heterosexual couples. This is different from the route and timing of HIV transmission in MSM. New HIV infections in MSM principally occur in chains of acutely HIV-infected highly sexually active young men, in whom acquisition and transmission are correlated in space and time. By the time TFP renders its effects, most new HIV infections in MSM will have already occurred. On a global level, less than 6% of all reports regarding the HIV care cascade from 1990 to 2016 included MSM, and only 2.3% concerned MSM in low/middle-income countries. Only one report originated from Asia Pacific. Generally, HIV cascade data in MSM show a sobering picture of TFP in engaging and retaining MSM along the continuum. Widening the cascade with a preventive extension, including pre-exposure prophylaxis, the first proven efficacious and only biomedical HIV prevention strategy in MSM, will be instrumental in achieving HIV epidemic control in this group.
- acquired Immunodeficiency syndrome
- HIV
- prevention and control
- pre-exposure prophylaxis
- antiretroviral therapy
- sexual behavior
Statistics from Altmetric.com
- acquired Immunodeficiency syndrome
- HIV
- prevention and control
- pre-exposure prophylaxis
- antiretroviral therapy
- sexual behavior
Introduction
Current prevention and control efforts are ineffective in containing the spread of HIV infection among men who have sex with men (MSM) in Asia Pacific. The number of newly reported HIV infections among these men in the region has been increasing and the majority of transmissions is now in this population.1 2 The rising epidemic predominance of MSM is particularly present in metropolitan areas, characteristic for the development of this part of the world. These high population density areas attract and harbour large MSM communities, served by a growing number of physical and virtual businesses catering to their social, sexual and other needs.3–5 The HIV prevalence and incidence among MSM in these settings are among the highest reported around the globe.1 2 6–8 In Bangkok, for example, the HIV prevalence among MSM in surveillance has consistently been around 30% throughout the past decade.6 9–11 This implicates ongoing HIV reproduction at the replacement level, reflected in the high observed HIV incidence of 6 per 100 person-years among men enrolled in follow-up studies.8 Consequently, the Asian Epidemic Model estimated that in 2010, MSM already accounted for more than 50% of new HIV infections in Bangkok.12 In 2015, this proportion further increased to 60%, and if new HIV infections in male sex workers and transgender women (TGW) were included, more than 80% of all new HIV infections were attributable to male-to-male sex.12 In another metropolis, Manila, 80% of newly reported HIV cases are currently in MSM and residents of the capital. In 2008, the daily number of newly diagnosed HIV infections was one, in 2010 three and in 2015 more than 18 cases per day.13 In parallel, the yearly reported number of new HIV infections in MSM doubled every 1.5 to 2 years, from 342 in 2008 to more than 7000 cases in 2016.13 If this trend is not reversed, 80 000–100 000 MSM will be HIV diagnosed and reported by the end of this decade.14 Similar epidemics are found in other urban settings in the region, such as in Jakarta, Kuala Lumpur, throughout Taiwan, and mainland China.15–19
These disturbing trends materialise against the background of a decline in the overall number of HIV/AIDS cases and increased uptake of highly active antiretroviral therapy (ART) as part of treatment for prevention (TFP).20 21 The latter strategy has been promoted as the pathway to the effective control of the HIV epidemic and creation of an AIDS-free generation.22–26 In response, major international donor agencies and funding alliances have adopted TFP as the core paradigm informing their grant portfolios and support decisions.27–29 This has led to an almost universal focus of national programmes and HIV prevention efforts on case finding, that is, identifying HIV-infected people, linking them to HIV treatment and care and reducing HIV viral load mediated onward transmission. Although the overall epidemic development associated with this focus appears to be positive,20 21 the HIV epidemic in MSM is continuing without any signs of decline or reversal.1 2 16 30 31 This raises doubt about whether TFP as a blanket approach across all risk groups is the right method to stop the HIV epidemic in MSM. Given the apparent lack of impact of TFP in this population, a critical review of this strategy and its results is justified. Possibly, the TFP strategy may need to be reconsidered or supplemented by other approaches to exercise more preventive effect. In this paper, we review currently available biomedical HIV prevention strategies, national HIV prevention policies and guidelines from selected countries in Asia Pacific, and review published data on the HIV care cascade in MSM. Finally, we demonstrate an alternative HIV prevention strategy which may be more effective in reducing the spread of HIV infection in this population.
Methods
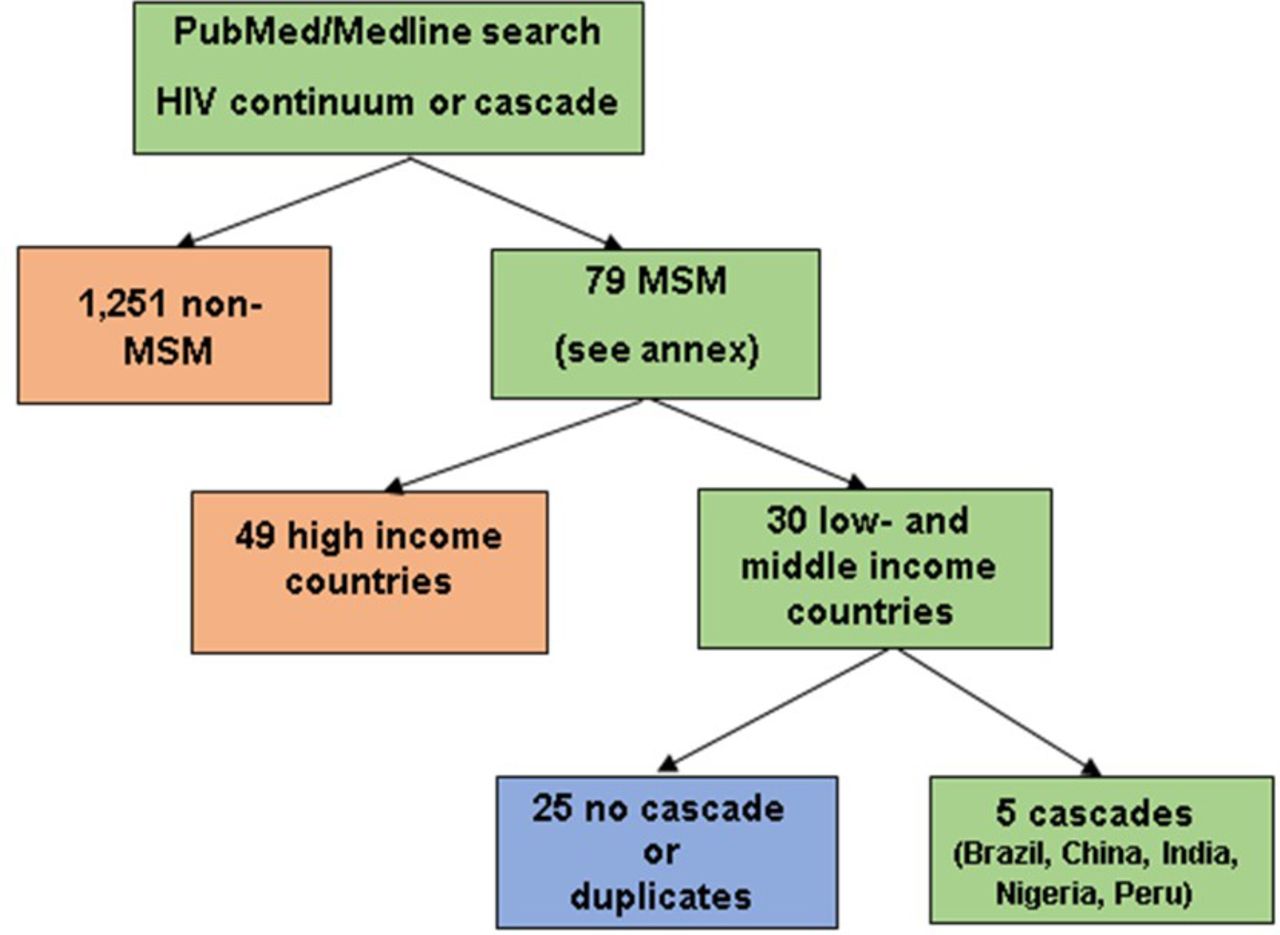
Review of available biomedical HIV prevention literature published in peer-reviewed English language scientific journals, announcements of funding opportunities and calls for proposals from international donor agencies and relief programmes such as the Presidents’ Emergency Program for AIDS Relief, the Bill and Melinda Gates Foundation and the Global Fund to Fight AIDS, Tuberculosis and Malaria. Scientific publications regarding the engagement of MSM in the HIV care cascade were reviewed by a systematic search of the PubMed/Medline database.32 Initial search terms used were ‘HIV’, ‘cascade’, ‘continuum’, ‘men who have sex with men’, ‘MSM’, ‘Asia’ and ‘Pacific’. This returned only three reports, one of which was a duplicate. After removing ‘MSM’, ‘Asia’ and ‘Pacific’ from the list, 1 330 entries were returned, of which 79 (5.9%) concerned MSM (figure 1 and online supplementary annex). Of the latter, 30 (38.0%) reported data from low/middle-income countries, of which five (16.7%) reported HIV cascade data. Twenty-five did not present such data or were duplicates. The five papers reporting MSM HIV cascade data originated from Brazil, China, India, Nigeria and Peru.33–38
Supplementary file 1
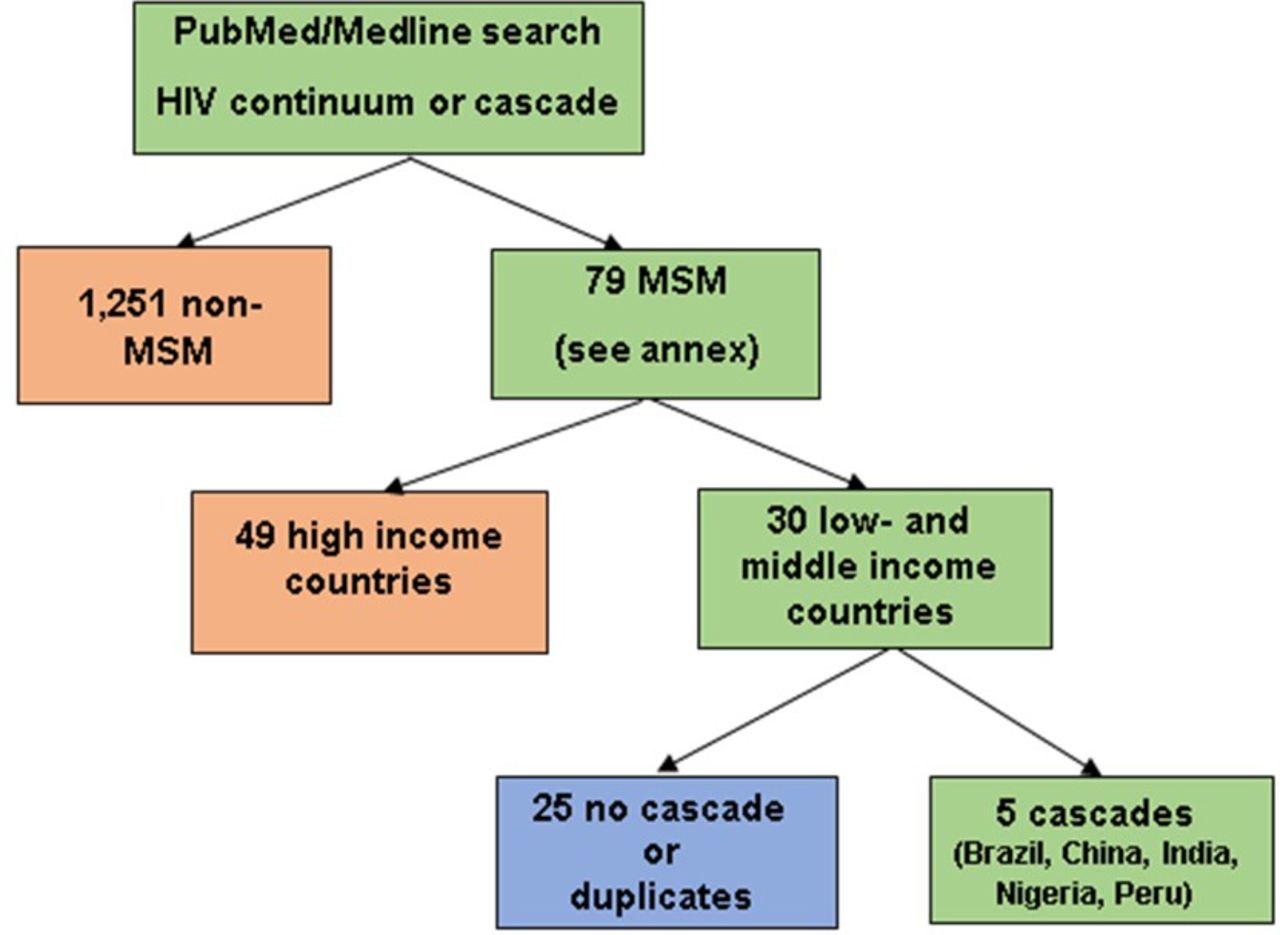
Schema of entries returned by PubMed/Medline regarding the HIV care continuum or cascade in men who have sex with men (MSM), 1990–2016.
Results
Antiretroviral HIV prevention
Grounded in phase III efficacy trials, highly effective HIV prevention modalities using oral antiretroviral (ARV) drugs profoundly changed the HIV prevention and treatment landscape. Eventually, these findings led to optimism about HIV eradication and the end of AIDS.39–43 The International Pre-Exposure Prophylaxis (IPrEX) study, evaluating daily oral dual ARV pre-exposure prophylaxis (PrEP) in MSM, was first to show preventive efficacy (44%).44 These results were rapidly overshadowed by the HIV Prevention Trial Network (HPTN) 052 Study of immediate initiation of ART, showing a 96% efficacy in preventing within-heterosexual couple HIV transmission.45 PrEP efficacy using oral mono and dual ARV drugs was subsequently shown in high-risk heterosexual men and women and persons who inject drugs.46–48 More recent clinical and pharmacological studies have demonstrated close to 90% protection of less than daily intake of dual oral PrEP in MSM.49–51
Since the number of CD4+ cells at time of presentation for care had not increased in the industrialised world since the introduction of highly active therapy in 1996,52 53 the HPTN 052 results formed a significant boost for the roll-out of earlier initiation of ART. Reformulated as TFP,45 54–59 early use of ART was encouraged as improving the health and longevity of the HIV infected, while at the same time preventing onward transmission. If implemented widely and thoroughly, it was argued that this strategy would implicate the end of AIDS.22–26 Since HIV treatment was imperative, the TFP ‘package deal’ of treating while preventing and vice versa, at relatively little or no extra cost, presented a policy option difficult to ignore or reject by most countries, including those in Asia Pacific. Guided by expanded US Department of Health and Human Services HIV/AIDS treatment guidelines, and supported by international donor agencies,27 28 59 most countries in the region implemented the ‘double-sided sword’ of TFP as a logical and acceptable HIV treatment, prevention and control strategy (table 1). While the initial focus of TFP was on early treatment (ie, <500 CD4+ cells), after clinical studies showed increased survival benefit of starting therapy as early as possible, universal access to ART guidelines widened TFP’s catchment area to include all HIV-infected individuals regardless of CD4+ cell count.59
HIV treatment and prevention policies, guidelines and implementation in selected countries in the Asia Pacific
TFP in MSM
No evidence for efficacy of TFP in protecting MSM from HIV infection is available. Hence, the rationale for TFP in MSM is based on assumptions about biological plausibility and external validity of efficacy found in heterosexual couples, that is, penile–vaginal intercourse during the HIV latency period.60 This is different from the principal route and timing of HIV transmission in MSM. Anal intercourse among men is multiple times more efficient in transmitting HIV infection than is vaginal intercourse,60 61 and this efficiency is further increased during acute HIV infection (AHI). Observational research in HIV-discordant MSM couples has shown that latency period anal HIV transmission is unlikely when HIV RNA viral load in the infected partner is undetectable.62–65 However, this observation does not account for differences in HIV transmission risk during AHI, when HIV viral replication and expression are the highest. A range of phylogenetic studies has shown new HIV infections in MSM principally to occur in chains of acutely HIV-infected highly sexually active young men, in whom acquisition and transmission are correlated in space and time.66–70 This incongruence between HIV epidemic properties and TFP protective realities has significant ramifications for the appropriateness of TFP as a blanket approach across key populations, including MSM. Unlike in heterosexuals, by the time TFP is initiated and renders its effects, most new HIV infections in MSM will have already occurred. Therefore, PrEP, the first proven efficacious and only biomedical HIV prevention strategy in MSM, with its focus on the HIV uninfected, should play an essential role in achieving HIV epidemic control in this group. However, in most countries with MSM-predominant epidemics in Asia Pacific, PrEP interventions have not been prioritised and are yet to become part of national guidelines and programmes (table 1).
The HIV care cascade
The HIV care cascade has been put forward as the single unifying conceptual framework to design, implement and evaluate the success of TFP in achieving an AIDS-free generation.22–27 It presents a deterministic model of discrete, consecutive stages of HIV treatment and care, starting with the proportion of HIV-infected individuals diagnosed, followed by proportions linked to HIV treatment and retained as part of eligibility evaluation for ART, receiving ART and being HIV RNA viral load suppressed. The HIV cascade was first implemented in the general HIV-infected population in the USA, and subsequently disaggregated in key populations in that country. Evaluation of the 1.15 million HIV-infected persons across the USA in 2009 revealed that 63.3% was either not diagnosed (18.1%) or diagnosed but not retained (45.2%), 4.1% was retained but not on ART, 7.3% was on ART but not virally suppressed and 25.3% was on ART and virally suppressed.71 Of the estimated 45 000 HIV transmissions during that year, in 91.5%, the source was undiagnosed (good for 6.6 HIV transmissions/100 person-years (PY)) or diagnosed but not retained (5.5 transmissions/100 PY).71 In line with these troublesome results, evaluations of the cascade among US-based MSM have shown an even less favourable picture. When the overall cascade was broken down by age and ethnicity, young and black MSM were found to be under-represented at every cascade step, including viral suppression.72 73 Hence, disaggregation of the cascade seems essential to sensitively evaluate access, uptake and impact of TFP among the most vulnerable and affected.
The HIV care cascade in MSM
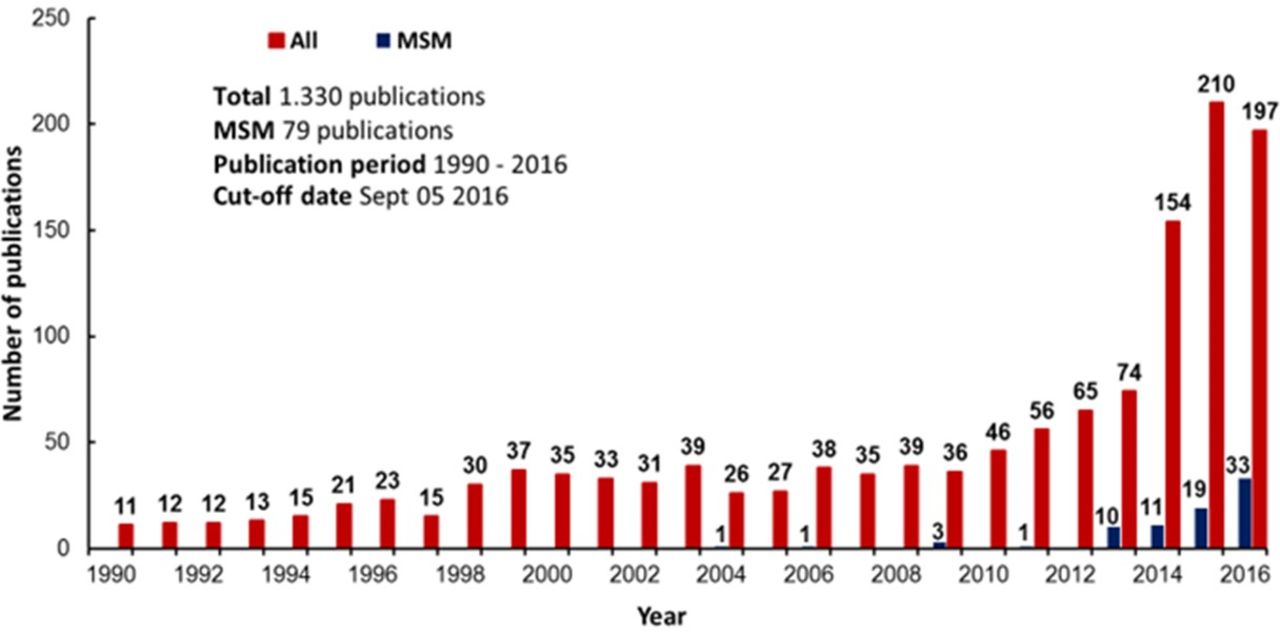
During the past two decades, the number of articles published in the peer-reviewed literature on topics related to the HIV care cascade or continuum strongly increased (figure 2). However, far fewer articles on MSM were found, as compared with heterosexuals and other groups, and even fewer articles on MSM were from low/middle-income countries. In the systematic review, we found only five articles—from Brazil, China, India, Nigeria and Peru—containing some HIV cascade information in MSM (table 2).33–38 Even so, all these cascades had missing information and, except for Peru, proportions of MSM virally suppressed were inflated by taking the number of diagnosed men to calculate subsequent proportional inclusions. Generally, proportions of virally suppressed MSM were low, except in a cohort study among MSM from Brazil (table 2).35

Frequency of entries returned by PubMed/Medline regarding the HIV care continuum or cascade, by risk category and calendar year, 1990–2016. MSM, men who have sex with men.
Summary of low and middle income country studies reporting MSM HIV care continuum or cascade data, returned by PubMed/Medline, 1990–2016
The double-sided HIV care cascade
While the HIV cascade may be a helpful tool to implement and monitor the delivery of HIV treatment and care for the overall HIV-infected population, it does not provide a similar mechanism for preventive services among those at risk. Figure 3 presents a double-sided cascade applied against data collected in the ongoing Test and Treat Study among MSM/TGW in various cities in Thailand. The cascade starts with HIV testing and entry in the preventive (left) or the therapeutic (right) cascade, depending on the test outcome. The therapeutic cascade is unidirectional with suppressed HIV viral load as the final stage, whereas the preventive cascade is circular (12-month cycles), with preservation of HIV-uninfected status as the desired cyclic outcome. The Test and Treat Study offers a variety of tailored HIV preventive services, including PrEP, dependent on risk profile and needs, for those who test HIV uninfected at entry and immediate linkage and access to HIV ART among those who test HIV infected. In brief, 131 (16.2%) out of 808 MSM/TGW tested HIV infected at entry during 2013–2015, of whom 90.8% were linked, 87.8% were retained, 65.6% were on ART and 63.4% were virally suppressed. Of the 677 (83.8%) MSM/TGW who tested HIV uninfected at baseline, 94.5% were linked to preventive services, that is, evaluation for PrEP, receiving PrEP, risk reduction counselling and STI and HIV retesting. Of the total, 92.6% initiated such preventive services, 74.9% were retained and 73.0% tested preserved HIV uninfected after 12 months (figure 3). Proportions of HIV infected and uninfected in different cascade stages are not fixed and evolve over time as new persons enter and others leave. This example from Thailand shows a simple and workable extension of the HIV cascade by integrating HIV therapeutic and preventive services.

{kind=link}
{kind=link}
{kind=link}
Double-sided HIV cascade among men who have sex with men and transgender women enrolled in the Thai Test and Treat Project, 2012–2015. ART, antiretroviral therapy.
Discussion
Despite the lack of empirical evidence for TFP to be efficacious in preventing HIV infection in MSM, most countries in Asia Pacific employ this approach as a blanket HIV prevention and control strategy across key populations. Phylogenetic studies convincingly show incongruence between the potential preventive impact of TFP and timing of HIV transmission in MSM. On a global level, less than 6% of all reports regarding the HIV care cascade from 1990 to 2016 included MSM, and only 2.3% concerned MSM in low/middle-income countries. Only one report originated from Asia Pacific. With exception of Brazil, countries from which HIV cascade data in MSM were reported show a sobering TFP success picture in engaging and retaining MSM along the continuum. However, the Brazil data were collected in the context of a cohort study, a protocol driven follow-up situation, different from regular provision of HIV treatment and care services.
The lack of inclusion of MSM as a priority population in national programmes and guidelines and their absence from scientific evaluations is particularly disappointing since PrEP, a biomedical intervention with proven efficacy, is available but left unused in most situations. Ideally, HIV cascade information regarding proportions of MSM virally suppressed could be used to prioritise communities in need of PrEP, but at present, this is far from reality.
Because both PrEP and TFP use ARV drugs, it has been argued that such drugs are for treatment and their use for prevention would go at the expense of access to such medication by those with HIV infection. Since TFP is already using ARV drugs for prevention, this no longer seems to be a valid argument. It would be more realistic and practical to see the use of ARV drugs on a continuum for prevention and treatment during different stages of risk versus disease. If not used for HIV prevention when indicated, indication may change to treatment at later stages. The double-sided cascade used in the Test and Treat Project in Thailand where ARV drugs are offered by indication for prevention or treatment provides an example of how this can be achieved. Not all who test HIV negative are offered or accepting PrEP in this approach; this depends on the eligibility, needs and wants of the individual. The difference here is that prevention precedes treatment or before the occurrence of disease, in line with conventional public health paradigms.
In previous reviews, the lack of epidemic response in MSM was largely attributed to obstructions in accessing HIV testing, treatment and care associated with structural factors, such as stigma and discrimination.74 75 Such obstructions may indeed hinder timely access and uptake, but our evaluation suggests the presence of a much wider problem, that is, a disconnect of HIV prevention efforts and HIV epidemic realities in MSM expressed in an under-representation in national programmes and in the scientific evaluation of HIV epidemic control policies. TFP is currently placed at the highest priority for HIV prevention and control on a global level. Less affluent countries have been receiving increased international donor support and programmatic assistance in rolling out and improving access to ART for those with HIV infection.76 However, as was shown in this review, TFP does not work as intended for populations of MSM in Asia Pacific, and may also not work for MSM and other key populations elsewhere. Therefore, key players, including international donors and governments, should reinvigorate HIV prevention efforts and integrate these into the HIV cascade; most importantly, they should embrace PrEP—the first proven and currently only biomedical HIV prevention strategy found efficacious in MSM—as an equally viable and imperative preventive measure for the HIV uninfected as is the condom. Inclusion of PrEP into national guidelines and programmes and making it universally available and accessible is an important first step to preventing new HIV infections and controlling HIV epidemics among MSM. Urgent next steps would be to develop and implement innovative strategies to speed up PrEP access and uptake, and to support PrEP adherence. Donors should make funding available for these endeavours and researchers should take on these tasks to improve and expand the HIV cascade equally across those at risk for HIV infection and those at risk for HIV disease.
Key messages
Antiretroviral treatment for prevention and its overriding conceptual framework, the HIV care cascade, appear to be ineffective in containing the spread of HIV infection in men who have sex with men (MSM).
Few reports evaluating the cascade among MSM in lower/middle-income countries show a sobering picture of engaging and retaining men across the continuum.
Preventive antiretroviral pre-exposure prophylaxis should play a more important role in achieving HIV epidemic control in this population.
References
Footnotes
Handling editor Jackie A Cassell
Contributors FVG conceptualized the review and wrote the first draft of the paper. TG performed the literature search. NP, JWDLVW, SS and YRL provided country-specific and regional information. NP also contributed data from the Thai Test and Treat study. All authors critically reviewed and commented on the manuscript draft. FVG compiled and submitted the final version of the review. The protocol of the Thai Test and Treat Study was reviewed and approved by the Ethical Review Committee of Chulalongkorn University, Bangkok, Thailand (OHRP IRB No. 00001607, Certificate of Approval No. 529/2013).
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.