Article Text

Abstract
Three randomised trials demonstrate that voluntary medical male circumcision (MMC) reduces male HIV acquisition by 50–60%, and post-trial surveillance has shown that the effects are long lasting. Scale-up of services has been initiated in 14 high-priority sub-Saharan African countries with high rates of HIV and low prevalence of MMC. However, circumcision coverage in the region remains low. Challenges to MMC rollout include suboptimal demand among higher-risk men, the need to expand access and reduce costs of MMC through personnel task shifting and task sharing, assuring and maintaining a high quality of service provision, and the testing and introduction of non-surgical devices. In addition, early infant male circumcision has not been adequately evaluated in Africa. Here, we describe challenges to implementation and discuss the ongoing and future role of implementation and programme science in addressing such challenges.
- CIRCUMCISION
- AFRICA
- HIV
Statistics from Altmetric.com
Introduction
Three randomised trials in Orange Farms (South Africa), Kisumu (Kenya) and Rakai (Uganda), reported that medical male circumcision (MMC) reduced the risk of HIV acquisition by over 50%.1–3 Post-trial follow-up of study participants in Kenya and Uganda,4 ,5 and population-based assessment of HIV incidence, comparing circumcised and non-circumcised men, indicate the effectiveness of MMC for HIV prevention in non-trial settings.6 ,7 Additionally, multiple observational studies, largely of men circumcised in childhood, support these findings.8 ,9 The trials and observational studies also suggest the MMC reduces the incidence of herpes simplex virus type 2 (HSV-2) and human papillomavirus (HPV) infections,10–12 and genital ulceration in men.13 In female partners, circumcision was found to reduce trichomonas, bacterial vaginosis, HPV and genital ulceration.14 One trial reported that MMC did not affect HIV acquisition in female partners over a period of two years,15 but modelling suggests that if male HIV prevalence is reduced by MMC, it will reduce female exposures and, thus, indirectly reduce infection in women.16 ,17
On the basis of the trials, the UNAIDS/WHO18 recommended MMC as an integral component of HIV prevention strategies in 2007. The agency set a goal of providing MMC to 20.3 million men in 14 priority southern and eastern African countries by 2015 in order to achieve 80% coverage, with a further 8.42 million procedures between 2016 and 2025 to maintain the 80% coverage.16 ,19 It is estimated that if targets are achieved, it could avert ∼3.36 million new HIV infections by 2025 at a cost of US$2 billion, producing a net saving of ∼US$16.51 billion by averted treatment and care costs.19
Since 2007, most priority countries have adopted policies promoting MMC.20 ,21 However, as of the end of 2010, fewer than 600 000 MMCs, representing less than 3% of the 20 million goal, had been achieved in the region.20 Only Kenya, with approximately 290 000 MMCs is on track to achieving its target with ∼61.5% coverage.22 Manifestly, substantial programmatic changes are needed. Implementation Science, as defined by Padian et al23 ,24 is research designed to promote the integration of research findings into policy and practice in order to improve the uptake, implementation and translation of evidence-based interventions. Here, we discuss implementation and programme science research findings related to MMC and additional research needed to help overcome challenges to scale-up of MMC programmes. Because MMC was only recommended for HIV prevention in 2007, there is limited programmatic experience. Moreover, we have little experience with the use of surgery for prevention of infectious disease. As a consequence, more emphasis has been placed on implementation science within vertical service delivery systems, rather than on programme science promoting collaboration and integration between programmes.
Optimising service provision
There are three conventional surgical methods for adult MMC: the forceps guided procedure, the dorsal slit and the sleeve procedure. The forceps guided method is simplest and requires the least surgical time (∼19 min), whereas, the dorsal slit is estimated to take approximately 21.5 min, and the sleeve procedure requires ∼27 min.25 Recent observations from Uganda suggest that clinical officers require ∼10–15 min for the dorsal slit procedure (G Kigozi, personal communication). In Rakai, the dorsal slit procedure was found to be simpler for trainees and to require less surgical time than the sleeve method.26 However, the duration of the surgery depends on the experience of the personnel: the time needed is substantially longer with newly trained clinicians (35–40 min).26 Approximately 100 procedures are required to reach optimum proficiency.27 ,28 In the three randomised controlled MMC trials, complication rates were comparable with rates of moderate to severe adverse events requiring treatment ranging from 1% to 3%,1 ,2 ,29 even though each site used a different surgical method. In the subsequent Kenyan service programme, the rate of observed complications was 1.9% as a proportion of all surgeries performed,30 Additionally, in Kenya, MMCs performed by non-dedicated providers were associated with increased adverse events.w1 An implementation science study in Rakai, Uganda, found that clinical staff responsible for general medical care had difficulties scheduling and dedicating time for MMCs in their work days (Kighoma pc). Thus, it is more efficient to employ a smaller number of dedicated clinical providers who have substantial experience, rather than a large number of less experienced operators who have multiple tasks.
Because the ratio of physicians to population is low in sub-Saharan Africa (0.16/1000), it is necessary to use lower echelon personnel, such as clinical officers and nurses, to meet the demand for services.w2 Studies in Uganda suggest that clinical officers are comparable to physicians in terms of safety, but require slightly more time to complete the procedures.26 WHO has recommended the Models for Optimising Volume and Efficiency (MOVE) strategy, originally developed in Orange Farm, South Africa, to increase throughput of patients and reduce the time demands on scarce skilled personnel.25 MOVE incorporates task shifting from physicians to lower-level clinicians and task sharing. In this approach, the lower-level personnel are responsible for preoperative preparation and anaesthesia, the ‘surgeon’ performs the circumcision, achieves haemostasis and inserts primary sutures, with lower cadres completing the wound closure and dressing. In Orange Farm, the MOVE approach allowed a team of five nurses and one circumciser to perform up to 50 MCs per day.w3 Similar results were achieved in Zimbabwe,25 and in Kenya, the MOVE strategy has facilitated the provision of MMC to approximately 290 000 men between 2008–2011.22 The observed rate of MOVE complications in Orange Farm was 1.8%; however, one-third of patients did not return for follow-up, so this complication rate cannot be fully assessed.w3 A review of the studies which examined the safety of task shifting suggested that the rates of complications were similar among physicians and non-physicians.w4
An additional important observation in the Kenyan programme is that demand for MMC is not constant over time. Peaks of demand were observed during school holidays, requiring a Rapid Results Initiative, a short-term intensification of services which enlisted up to 700 providers to meet the demand.22 With respect to programme efficiency, clients who fail to come for scheduled MMC appointments can affect programme productivity, a problem which can be partially mitigated by use of cell phone text message reminders for surgery and follow-up visits (N Kighoma pc).
Service delivery may be further optimised through the use of MMC devices which can reduce surgical time to approximately 5 min. Two devices, the Shang ring and the PrePex, are being evaluated. The Shang ring was developed in China and has been used in ∼200 000 MMCs in that country. The Shang ring, applied under local anaesthetic, consists of a plastic inner and outer ring which are clamped over the foreskin; the latter is then removed surgically. The ring secures haemostasis and approximation of skin edges, and is removed after 7 days. The PrePex device consists of a firm plastic inner ring and an outer elastic band which compresses the foreskin leading to ischaemic necrosis of the distal preputial tissue. Since the foreskin is not excised at the time of PrePex placement, the procedure does not require local anaesthesia. The device is removed after 7 days and the necrotic tissue is trimmed under topical anaesthesia.
There are limited data on the safety of these devices. The Shang ring has been evaluated in China with reported adverse event rates between 1% and 3%, but the lack of diagnostic standardisation makes interpretation problematic.w5 One study of 486 men in Kenya reported rates of 1.3% for infection, 0.8% bleeding and 0.8% wound dehiscence (total 2.9%).w6 There are ongoing studies of Shang ring acceptability and safety in Kenya and in Rakai, Uganda. Preliminary data from the Rakai study suggest that the Shang ring is highly acceptable, with ∼67% of men choosing this method over conventional surgery using the dorsal slit. The moderate and severe adverse event rate declined with increasing experience of the providers, and was ∼0.5% after completion of the first 45 patients. (G Kigozi, pc)w7 Additionally, two participants (2.1%) attempted to remove the device on their own prior to the 7 day visit, despite preoperative education not to do so (one succeeded), but neither experienced wound dehiscence or another adverse event. Only one study of 55 men in Rwanda has reported on the PrePex device with one adverse event (1.8%).w7 However, this latter study was conducted in collaboration with the device manufacturer, and is too small to allow interpretation. Additional studies are underway.
Although these devices reduce the surgical time, and allow task shifting to non-physicians, both devices require follow-up for removal, adding to the programmatic burden and costs. Given the relatively modest rates of postoperative follow-up reported in service programmes (65–80%),22 w8 failure to return for ring removal could be problematic and methods of encouraging men to come for scheduled visits need additional assessment. With respect to cost, the Shang ring currently costs ∼$15.00 and the PrePex $20.00; although costs are likely to decline with wider adoption, the overall cost saving compared with conventional surgery (∼$45–65) may be substantial.19
Most efforts to scale-up MMC services have found that static facilities, such as hospitals, experience declines in demand over time as the catchment population motivated to accept the service became saturated. Moreover, in rural settings with scattered populations, the use of static facilities increases transport time and loss of work time for participants, and often require overnight stays, increasing programme costs. Therefore, several programmes have used mobile MMC strategies, with surgery being performed in temporarily equipped health centres, tents or mobile vans.22 w8 The Rakai experience with mobile camps has been encouraging with 300 surgeries performed per week and low rates of complications (G Kigozi, pc). If preliminary safety data on the Shang and PrePex devices are confirmed, the use of devices could substantially facilitate a mobile service approach.
Early infant male circumcision
Early infant male circumcision (EIMC) is simpler, safer and less expensive (∼$5.0–10) than adolescent or adult MMC, but has received less attention because the priority has been to maximise MMC among sexually active men to realise a short-term impact on the epidemic.w9 Observational data suggest that MMC in infancy/childhood is highly protective against adult HIV.9 Currently, HIV incidence among Rakai men circumcised in infancy is 0.5/100 py compared with 1.1/100 py in uncircumcised men.7 Thus, EIMC may be a highly effective approach to increasing long-term MC coverage for the benefit of future generations.17 Also, EIMC avoids the challenges associated with adult resumption of intercourse prior to complete wound healing (reported by 28% of married and 7% of unmarried men in the Rakai MC trials),29 and would cover men who might adopt higher risk behaviours in adulthood – the crucial group with lower rates of adult MC adoption.7
There has been limited implementation science research on EIMC in sub-Saharan Africa. A Botswana trial in neonates compared the Mogen clamp to the Plastibell methods of surgery performed by physicians in a hospital setting; local anaesthesia was provided via EMLA cream.w10 w11 There were no adverse events with the Mogen clamp, but in two out of 50 infants (4%) circumcised with the Plastibell, the rings were retained and required removal by trained personnel. The investigators concluded that the Plastibell was not appropriate for an African programmatic setting.w11 Two other studies of EIMC provided by physicians are ongoing in Swaziland and Zambia, and both report that the Mogen clamp appears to be the most appropriate method for the African setting (Elizabeth Stringer, Kelly Curran, personal communication).
The provision of services for neonates presents challenges to service delivery, because births often occur in the home or in decentralised sites, with minimal medical supervision. Research on EIMC provision by midwives, including studies to determine appropriate training for such persons, is thus urgently needed. At this time, midwives are not licensed to perform the procedure in most southern and East African countries.
A high proportion of African parents say that EIMC would be acceptable for their sons.w12 However, in Botswana, despite a reported acceptability of more than 90%, only 63% of parents opted to have their infant son circumcised.w11 It is likely that the lower uptake reflects the fact that mothers had not received adequate counselling on EIMC during antenatal care. The need to obtain paternal agreement was an additional impediment to acceptance. Another concern is that parents do not realise that the neonatal period is a safe time for EIMC, and may believe that the procedure is best performed in older babies and toddlers who are perceived as being ‘stronger’. (R Plank, pc) However, EIMC is more difficult in older children,w13 and parents need to be informed that the optimal age for infant surgery is less than 2 months.
Demand creation
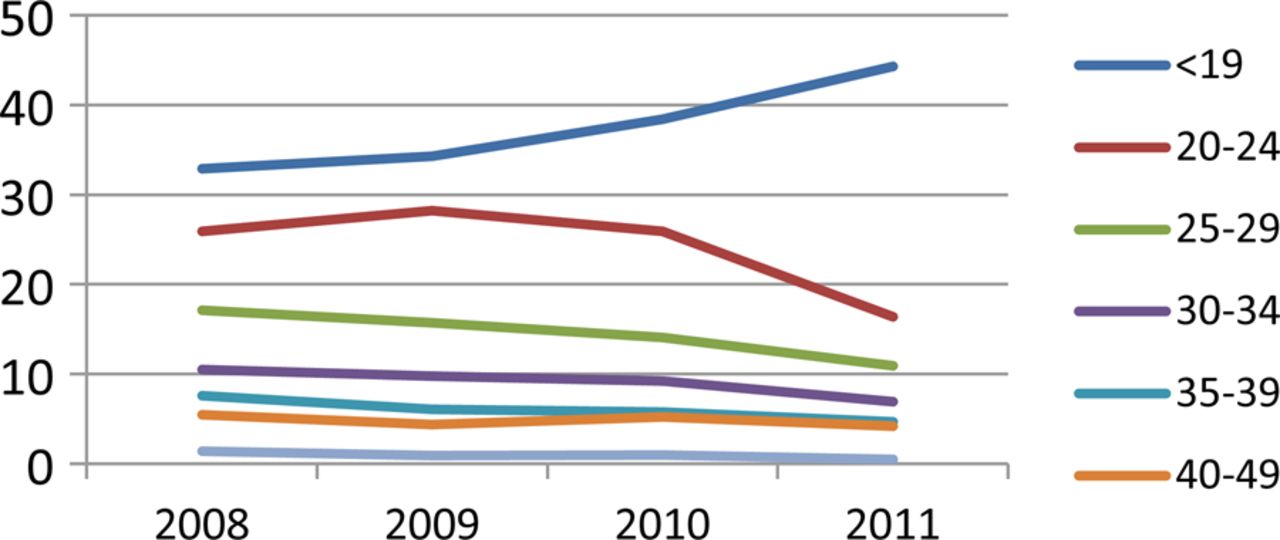
Surveys in sub-Saharan Africa suggest that around 65% of men say that they would be willing to accept MMC (range 28–87%).w12 w14 However, as noted earlier, the uptake of MMC has been low in most programmes, with the exception of Kenya.19 Males are also under-represented in HIV testing, treatment and care programmes,w15 w16 suggesting that the disinclination of men to access healthcare may be partially linked to perceptions of masculinity.w17 w18 Several MMC programmes have reported an over-representation of younger low-risk adolescents. For example, in Iringa, Tanzania, 75.7% of MMC clients were adolescents under 19 years of age,w8 and in Kenya, around 70% were 19 years or less.30 In Rakai, Uganda, there has been a progressive increase in the proportion of MMC acceptors who are adolescents <19 years, with a decline in the proportion of older, higher-risk men (figure 1). Clearly there is need for programmes to target older and higher-risk men, although strategies to accomplish this have not yet been developed and tested. Ongoing qualitative studies in Rakai are assessing barriers and facilitators to the acceptance of voluntary medical male circumcision in order to develop appropriate interventions.

The age distribution of VMMC acceptors in Rakai, Uganda. 2008–2011. Access the article online to view this figure in colour.
The prevalence of male circumcision in the general population of the 50 villages in the Rakai Community Cohort study (RCCS) increased from ∼20% in 2002–2003 (almost all among Muslims), up to 46.7% in 2010. Among non-Muslim men, the prevalence of MMC rose from ∼4% to 35.0% in 2011 as a consequence of the randomised trial and post-trial MMC services.7 In Nyanza Province of Kenya, the prevalence of VMMC increased from 55% in 2009 to 84% in 2010.22
Qualitative studies suggest that reasons for non-acceptance of VMMC include fear of pain, concerns over sexual potency and dysfunction, and time lost from work.w19 Anaesthesia and analgesia are critical for MMC acceptability, and an implementation science trial in Rakai showed that a mixture of lignocaine and bupivacaine provided better intraoperative and postoperative pain control compared with lignocaine alone.w20 Empirical studies indicate that male potency and sexual satisfaction are not adversely affected by MMC,w21 w22 and female sexual satisfaction was found to increase after the male partner's circumcision.w21
Strategies for demand creation are not well developed.w23 Most programmes employ community mobilisation, use of mass media, and many include women in their outreach.22 w2 w3 w8 In Rakai, men tend to attend community mobilisation meetings less than women, suggesting that in some populations, such outreach may not be the most effective for MMC promotion. However, most men have access to mass media, such as the radio, and many have cell phones. Programmes also target specific periods for intensive demand creation, such as school holidays, the end of harvest or the cool season.22 w8 However, there has been little empirical implementation science studies to determine the most effective strategies to increase acceptability and demand. The randomised trials compensated participants for enrolment and follow-up, and this was thought to enhance recruitment and retention. Conditional cash transfers have been effective to improve utilisation of preventive health services in poorer countries,w24–w26 but there are no data on the use of conditional cash transfers to promote7 MMC.
Evaluation of coverage and effectiveness and impact of MMC on HIV incidence
The randomised trials clearly demonstrated the efficacy of VMMC for HIV prevention in men. However, there is less evidence of effectiveness. A post-trial study from Kenya reported that HIV incidence was reduced by 64% in circumcised men over 54 months of observation suggesting prolonged effectiveness of MC.w27 Following trial closure of the Rakai MMC trial, circumcision was offered to control arm participants, and post-trial surveillance was maintained for up to 4.79 years, while 78.4% of uncircumcised trial participants accepted MC following trial closure. In control arm participants, post-trial HIV incidence was 0.54/100 person years (py) among circumcised men and 1.71/100 py in uncircumcised men (adjusted effectiveness 67% (95% CI 38% to 83%) (figure 2). There were no significant differences in sociodemographic characteristics and sexual behaviours between controls accepting MC and those remaining uncircumcised. Long-term effectiveness can also be inferred from observational studies which show an association between MC, largely performed during childhood, and subsequent reduced HIV prevalence and incidence among circumcised adult men.9 w28–w32

{kind=link}
{kind=link}
Post-trial Kaplan–Meier survival analysis of incident HIV among control arm participants circumcised and uncircumcised after trial closure. Access the article online to view this figure in colour.
There have been two implementation science evaluation studies to empirically estimate the impact of MMC on HIV acquisition in the general population. In Orange Farms, South Africa, Auvert et al6 conducted two cross-sectional surveys of random samples of men aged 15–49 years in 2007 and 2010. The prevalence of MMC increased from 15.6% in 2007 to 49.4% in 2010. Using the 2010 survey, HIV incidence was assessed using the Calypte HIV-1 BED assay to detect presumptive ‘new’ infections within a window period of ∼15 months. HIV prevalence was 20% in uncircumcised men and 6.2% in circumcised men. Estimated HIV incidence in the 15–34-year age group was 2.86/100 py among uncircumcised and 0.42/100 py among circumcised men, with an adjusted incidence rate ratio of 0.20, 95% CI 0 to 0.55. The authors estimated that MMC accounted for a 61.0% reduction in incident HIV at the population level. However, there are concerns that the BED assay may not accurately estimate HIV incidence because of false positive results among persons with advanced disease or those on antiretroviral therapy. Additionally, self-reported circumcision was found to be highly unreliable in this population; 44.9% of men who said they were ‘circumcised’ were found to have intact foreskins.w33 This misreporting occurred because the word for ‘circumcision’ is the same as the word for ‘initiation’ in the local dialect, so men who had been initiated but not circumcised at initiation responded affirmatively to the question.
The Rakai Programme assessed coverage and impact on incident HIV in the general population of non-Muslim men enrolled in the RCCS. This cohort has maintained approximately annual surveillance in a population of ∼14 000 males and females aged 15–49 years, resident in 50 communities. The prevalence of MMC in non-Muslim men was ∼4% prior to the availability of services (mid-2004), and increased to 35.9% in 2010 after the availability of services. HIV incidence in non-Muslim men was 1.36/100 py during in the 2000–2003 period prior to the availability of MMC services, and declined to o 1.05/100 py in the 2008–2011 period, (adjusted incidence rate ratio=0.78, 95% CI 0.62 to 0.98, p=0.04). The population-attributable fraction of the contribution of MMC to the decrease in HIV incidence among non-Muslim men was 37.1%.7 There were no behavioural changes that could account for this decline in HIV incidence. During the same periods of time, HIV incidence among Muslim men remained stable (0.50/100 py in 2000–2003, and 0.55/100 py in 2004–2010), suggesting no secular trends. There was no significant decline in HIV incidence among non-Muslim women (1.39/1000 py in 2000–2003 and 1.20/100 py in 2004–2009, IRR=0.89, 95% CI 0.71 to 1.05, p=0.15).
MMC policies
Dickson et al20 assessed policy and programme implementation in the UNAIDS priority countries using a diffusion of innovation framework. They identified pilot demonstration programmes as most predictive of programme scale-up, along with a male circumcision ‘focal point’ in the health service structure, and a national policy and implementation strategy. National leadership was particularly important in Kenya, where the Luo who traditionally do not circumcise, were encouraged to adopt the practice by the Luo Council of Elders in Nyanza Province and by the prominent political figures, including the prime minister, Raila Odinga (himself a Luo), as well as the minister of health. Political leadership was also important in Botswana, Rwanda and Swaziland, but was absent or low in Mozambique and Uganda.20
The role of implementation science in MMC rollout
Implementation science has demonstrated strategies to make MMC more accessible and efficient. To date, the evidence suggests that even though medical training is not needed to provide safe MMC, specialised and experienced personnel are needed in order to minimise surgical time and complication rates. If ongoing research on MMC devices confirms earlier reports of safety and acceptability, Implementation Science studies will be required to determine the levels of practitioners who can safely deliver the services, as well as their training and supervision needs.
Demand generation represents a priority area for Implementation Science studies. Given the apparent reluctance among higher-risk men to accept medical services, including MMC for HIV and sexually transmitted infection prevention, multiple additional strategies to increase access and acceptability urgently need to be tested. These may include expanded clinic hours, male-only clinics, services aimed at particular age groups to avoid mixing of older and young males, and mobile services placed close to work sites. Additionally, increasing MMC acceptance may potentially benefit from ‘demedicalisation’ of the service, rendering it socially desirable rather than something that is solely ‘good for your health’. As indicated, fear of surgical pain and concern about reduced sexual pleasure are cited as barriers to MMC. Rigorous data from the MMC trials showed no decline in sexual satisfaction and function post-MMC, and increased satisfaction among women partners; interviews with MMC clients also indicated the adequacy of surgical pain relief. Thus, there is a need to test appropriate and culturally sensitive ways of disseminating these messages, potentially including testimonials by satisfied clients and women partners in the mass media.
Implementation science methods for research on MMC provision
Although classical randomised trials are desirable in some situations (such as, to demonstrate efficacy for HIV prevention or for direct comparisons of safety between MMC devices), much of the needed Implementation Science on MMC provision can be accomplished through careful observational and operations research, using approaches such as step-wedge designs, time-trend analyses and comparisons with data from the trials and subsequent programmatic studies. Compared with randomised trials, such approaches can be more rapid, better reflect realistic programmatic settings, and are generally less expensive. The Implementation Science approach is also more conducive to flexibility in the design of the MMC rollout, based on iterative analyses of effects to date. However, care must be taken to ensure this research is conducted rigorously, with clearly stated goals, defined evaluation methods, careful (and where appropriate, predetermined) data analyses and transparent interpretation and reporting of results.
Implications for program science
The MMC rollout experience to date has been greatly facilitated by effective utilisation of implementation research. However, other aspects of programme sciencew34 W35 have not received much attention in this effort. Programme Science as mentioned by Aral and Blanchard can be defined as ‘Promoting collaboration and integration between programs and science to improve the ways programs are designed, implemented and evaluated to accelerate and increase health impact.’ The emphasis in programme science is on the totality of a programme. As such, it focuses attention on interactions among interventions and between interventions and the context into which they are introduced.
Particularly salient in the programme science approach are issues of coverage and expansion of coverage (scale-up), especially among those who are most at risk for transmitting infection through carefully planned targeting. The latter necessitates in-depth study of the epidemiologic, social, economic, organisational and political context. The success of the MMC rollout in Kenya is, to a great extent, a result of the sociopolitical context in Kenya. An analysis of the organisational context in Uganda may help achieve more effective expansion of coverage among men at high risk of transmitting HIV. Programme science, including implementation research, can significantly enhance the impact of HIV/sexually transmitted infection prevention programmes.
Summary
Implementation Science has contributed to our knowledge of barriers to MMC provision and acceptance, coverage at the community level and in risk groups, and has provided early indications of population-level effects on HIV incidence. The current programmatic research focus will need to include maximisation of efficiency while maintaining safety, increasing access, and very importantly, generating demand to increase coverage, especially among subgroups at risk of HIV.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online references
Footnotes
-
Competing interests None.
-
Ethics approval Institutional Review Boards in Uganda and the US (The Scientific and Ethics Committee of the Uganda Virus Research Institute, #GC/127/12/09/01, the Uganda National Council of Science and Technology #HS 354, and Western IRB (Olympia, WA, #20030586).
-
Provenance and peer review Commissioned; internally peer reviewed.