Article Text

Abstract
Despite emergency and essential surgery and anaesthesia care being recognised as a part of Universal Health Coverage, 5 billion people worldwide lack access to safe, timely and affordable surgery and anaesthesia care. In Tanzania, 19% of all deaths and 17 % of disability-adjusted life years are attributable to conditions amenable to surgery. It is recommended that countries develop and implement National Surgical, Obstetric and Anesthesia Plans (NSOAPs) to systematically improve quality and access to surgical, obstetric and anaesthesia (SOA) care across six domains of the health system including (1) service delivery, (2) infrastructure, including equipment and supplies, (3) workforce, (4) information management, (5) finance and (6) Governance. This paper describes the NSOAP development, recommendations and lessons learnt from undertaking NSOAP development in Tanzania.
The NSOAP development driven by the Ministry of Health Community Development Gender Elderly and Children involved broad consultation with over 200 stakeholders from across government, professional associations, clinicians, ancillary staff, civil society and patient organisations. The NSOAP describes time-bound, costed strategic objectives, outputs, activities and targets to improve each domain of the SOA system. The final NSOAP is ambitious but attainable, reflects on-the-ground priorities, aligns with existing health policy and costs an additional 3% of current healthcare expenditure.
Tanzania is the third country to complete such a plan and the first to report on the NSOAP development in such detail. The NSOAP development in Tanzania provides a roadmap for other countries wishing to undertake a similar NSOAP development to strengthen their SOA system.
- surgery
- anaesthesia
- obstetrics
- health policy
- national health strategic plans
- global surgery
- national surgery anaesthesia and obstetric plans
- global health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- surgery
- anaesthesia
- obstetrics
- health policy
- national health strategic plans
- global surgery
- national surgery anaesthesia and obstetric plans
- global health
Summary box
Nine out of 10 people in low-income countries lack access to safe, timely and affordable surgery, anaesthesia and obstetric care.
Coordinated health system-based strategic plans are needed to improve the provision of surgery, anaesthesia and obstetric care.
This paper provides lessons learnt from the development of a National Surgical, Obstetric and Anesthesia Plan in Tanzania, which can be applicable to other countries looking to improve surgery, obstetric and anaesthesia systems as they move towards Universal Health coverage.
Introduction
In most low-income, and many middle-income countries, the provision of surgery and anaesthesia care is inadequate in quantity and quality.1 The Lancet Commission on Global Surgery (LCoGS) found that 65% of the world population currently lack access to safe, timely and affordable surgical and anaesthesia care and there is an unmet need for 143 million additional surgical procedures each year.1 In May 2015, through resolution 68.15, the WHO member states unanimously recognised the critical role of surgery and anaesthesia in achieving Universal Health Coverage (UHC), in which all people receive needed quality health services without the risk of financial hardship.2 Furthermore, improving access to surgical services has been shown to be cost-effective and addressing surgical care leads to significant economic gains in the long term.1 3
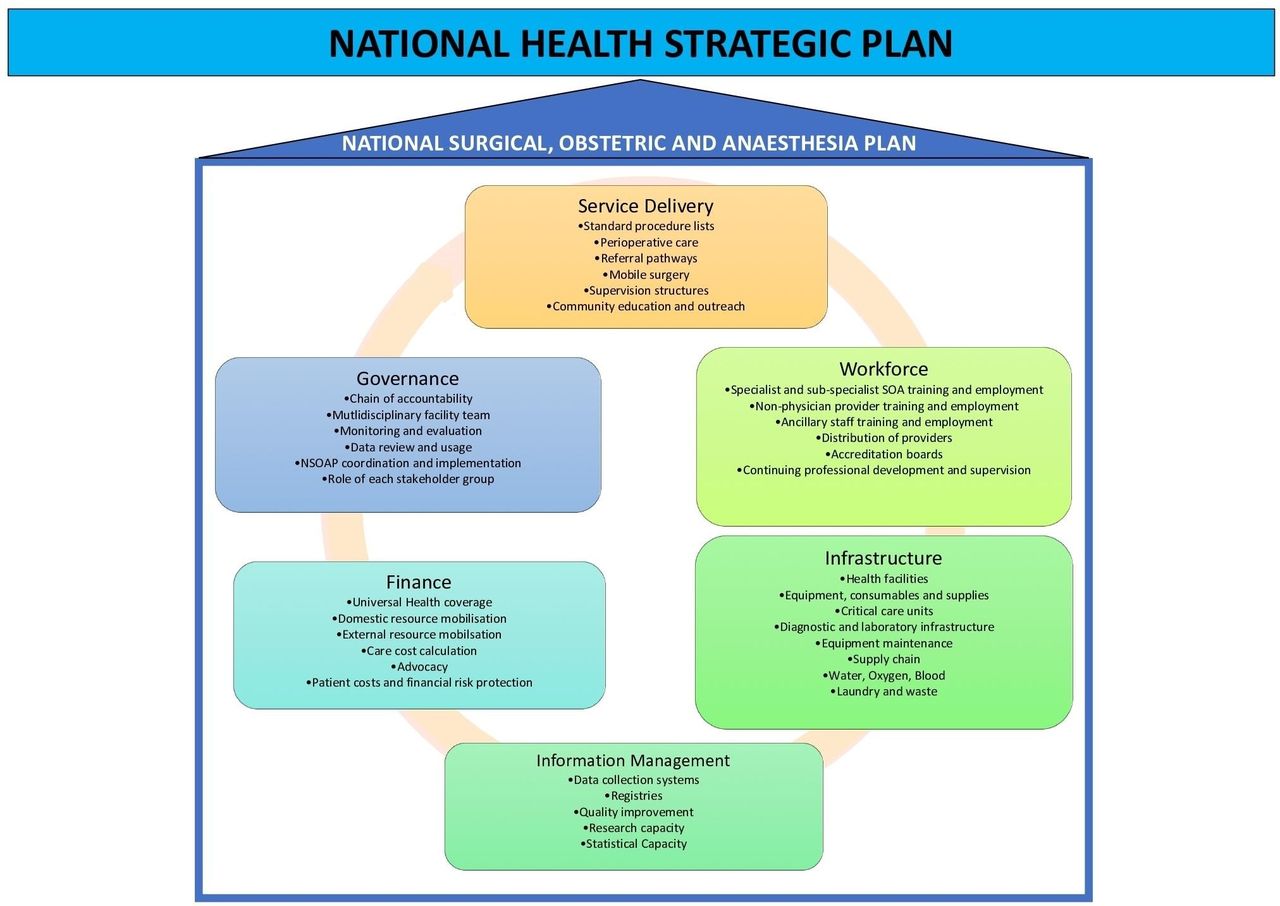
Surgical, obstetric and anaesthesia (SOA) are complex interventions each requiring a strong health system across each of six domains (figure 1) (Box 1) . They require a coalescence of the correct prehospital and preoperative, intraoperative and postoperative care. As an example, in the prehospital phase, they require a functioning referral system, including ambulance networks and appropriate protocols to safely refer and transport patients to higher levels, in order to get the patient to hospital in a timely way. Once in hospital, preoperatively, they require the appropriate level of critical care (The Intensive Care Society 2009 guidelines for ‘levels of Critical care for adult patients’ are used throughout when describing critical care4) to stabilise and resuscitate the patient, as well as laboratory staff and infrastructure to provide necessary tests and support in assessment of the patient’s condition; intraoperatively, the patient requires operating room infrastructure, equipment, blood, suture material, drugs and the specialist surgical, specialist anaesthesia and ancillary staff to carry out the procedure; and postoperatively, the patient needs postsurgical care, at times critical care, post-anaesthesia support, pain management, follow-up and, possibly, rehabilitation services. There needs to be sufficient management and governance to keep these functions in place, and the entire episode of care must be affordable such that patients are not impoverished by their care. Given the complexity and co-dependence of these domains, vertical programme aimed at a single domain (eg, infrastructure) are unlikely to have a sustained impact on the ability to provide timely, high-quality, safe and affordable SOA care. To coordinate a systematic improvement in all domains of the surgical health system, a strategic plan is required.1 5
Definitions
SOA system: the required service delivery protocols, workforce, infrastructure (including equipment and consumables), information management, financing and governance required to provide high-quality, safe, timely and affordable surgery, obstetric and anaesthesia care to a population. The items listed in figure 1 provide an example of what is included.
SOA care delivery: The provision of timely, high-quality, safe and affordable surgery, obstetric and anaesthesia care. The paper uses the WHO definition of high-quality care: ‘the extent to which health care services provided to individuals and patient populations improve desired health outcomes. In order to achieve this, health must be safe, effective, timely, efficient, equitable and people-centred’.29
SOA workforce: All personnel required to provide high-quality, safe, timely and affordable surgery, obstetric and anaesthesia care. It includes but is not limited to specialist surgeons, anaesthesiologists and obstetricians as well as specialist nurses, theatre nurses, nurse anaesthetists, physiotherapists, theatre managers, biomedical engineers and technicians, occupational therapist, social workers.
Critical Care: ‘Critical care refers to two related processes. Firstly, “critical” refers to discernment or recognition of a crucial and a decisive turning point, the deterioration of the patient’s condition, followed, secondly, by “care” that is, intervention including resuscitation and transport to a critical care service. Critical care resuscitation and treatment interventions include a complex range of general and specialty procedures, supports and diagnostic procedures. Thus, the critically ill patient benefits from appropriate and timely critical care in the health system with a greatly increased probability of survival’.30
Critical illness: ‘Critical illness is a life-threatening patient condition requiring critical care intervention for patient survival’.30
Strategic objective: Statement of a desired future state, condition or purpose, which an institution, a project, a service or a programme seeks to achieve.31
Output: These are the products or services required to achieve a strategic objective, which result from a series of activities. The distinction between strategic objectives and outputs is that strategic objectives are broader and may have several constituent outputs that are more specific.32
Activity: Specific actionable item to be implemented in order to achieve a particular output.32
Target: An intermediate result towards an objective that a programme seeks to achieve, within a specified timeframe, a target is more specific than an objective and lends itself more readily to being expressed in quantitative terms.31

Requirements for a comprehensive surgical, obstetric and anaesthesia system in each of the six health system domains. NSOAP, National Surgical, Obstetric and Anesthesia Plan.
A National Surgical, Obstetric and Anesthesia Plan (NSOAP), much like similar plans for Maternal and Child Health, HIV or malaria sits within the national health strategic plan of a country. It provides a costed multi-stakeholder consensus vision of the current situation of SOA services and provides a roadmap to improving SOA care delivery across each of the six domains of the health system: service delivery, infrastructure, workforce, information management, finance and governance (figure 1).
The development of NSOAPs can have number of positive impacts, namely priority setting, coordination and funding: (1) NSOAP development itself improves visibility and accountability around the SOA system, an otherwise neglected area of the health system.6 NSOAP development allows a country to collectively decide its priority areas and translate these into concrete implementable activities within an associated accountability structure (2) The NSOAP, once completed, ensures greater efficiency of existing resource allocation through improved coordination among government programme and private and civil society actors. This coordination avoids the invariably ineffective strategy of developing health system domains in isolation; for example, the building of new operating rooms (infrastructure) without consideration as to how they will be staffed (workforce). This improved coordination also avoids duplication of efforts, particularly as efforts to strengthen SOA care delivery overlap with efforts to improve the care of other conditions, such as maternity care and cancer care, and vice versa. (3) An NSOAP could be used to attract additional funding for SOA system improvements from international and domestic sources because programme developed in-country with clear strategic objectives, outputs, activities and targets make attractive funding proposals.7 Despite these advantages, a 2015 study of national health plans of sub Saharan Africa noted 63% of plans had less than five mentions of surgery and 33% had no relevant targets.6 By 2016, only three countries, Senegal, Zambia and Ethiopia had developed NSOAPs.8 9
Tanzania situation
In Tanzania, it is estimated that 19% of all deaths and 17% of disability-adjusted life years are attributable to conditions amenable to surgical treatment.10 11 However, access to SOA care delivery is limited. The surgical system of a country like Tanzania can be assessed using six core indicators proposed by the LCoGS. Of these six indicators, four have been published by the World Bank as World Development Indicators (WDIs). The WDIs for Tanzania in comparison to neighbouring countries are presented in table 1, the additional two LCoGS indicators of postoperative mortality rate and 2-hour access to Bellwether procedures (laparotomy, C-section, appendicectomy) are not presented as data are unavailable.
Current surgical capacity in Tanzania in comparison with regional neighbours measured by four WDIs
To address the deficiencies across the SOA system, illustrated in table 1, in 2018, the Tanzanian Ministry of Health, Community Development, Gender, Elderly and Children (MoHCDGEC) developed an NSOAP as a roadmap for SOA system improvement for 2018–2025. The NSOAP aimed to (1) reflect priorities of SOA system stakeholders, in particular frontline providers; (2) set ambitious yet attainable goals within the given timeframe and resources; (3) align with broader national health priorities; and (4) encompass activities of all actors spanning the public, private and non-governmental sectors. This paper outlines the methodology of developing such a plan, highlighting the strategic objectives, outputs and activities of the plan.
Section 1: NSOAP development
The first key step in the NSOAP development was the strong commitment from the MoHCDGEC. This commitment was confirmed in November 2016 with a directive from the Permanent Secretary of the MoHCDGEC to develop the NSOAP and an assignment for the NSOAP development to be led by the department of curative services. Due to the specific governance structure in Tanzania, coordination between two government entities was required from the beginning of the NSOAP development. In Tanzania, the Ministry of Health is primarily responsible for health policy, planning and training while the President’s Office, Regional Administration and Local Government (PO-RALG) is responsible for the implementation of health plans at the district level and below. As such, a PO-RALG representative was involved at every level of NSOAP development to ensure alignment of the NSOAP with implementation priorities.
The NSOAP development included four major steps: (1) situation analysis, (2) stakeholder engagement and priority setting, (3) drafting and validation and (4) costing (figure 2). The NSOAP development concluded with the plan’s official launch and adoption in March 2018. The NSOAP development was facilitated by the Programme in Global Surgery and Social Change at Harvard Medical School. It was important to all stakeholders and to the validity of the NSOAP that the Harvard team acted as only catalyst and were not responsible for proposing or shaping the priorities contained within the NSOAP. Instead their role was in assisting the MoHCDGEC with logistics to convene stakeholders, evidence and data gathering and collation and synthesis of priorities laid out by the stakeholders.

{kind=link}
{kind=link}
Summary of the NSOAP development in Tanzania. NSOAP, National Surgical, Obstetric and Anesthesia Plan.
Situation analysis
A situation analysis was conducted between November 2016 and March 2017 to better understand, quantitatively and qualitatively, the strengths and weaknesses of the current SOA system in Tanzania. This included a systematic review of all academic indexed literature, grey literature as well as all relevant government policies, policy guidelines and government data related to the SOA system in Tanzania. All relevant strategic objectives, outputs and activities from existing complementary MOHCDGEC plans, which may interact with NSOAP were identified and the system was mapped. As such, any new strategic objectives, outputs and activities proposed in the NSOAP could build on any other existing plans and avoid incongruity and overlap (eg, online Appendix 1).12 The results of this have been reported by Nyberger et al.13
Supplemental material
Challenged by the inherent publication bias in the available literature, which most often originated from larger teaching hospitals, the systematic review was supplemented with semistructured interviews with stakeholders involved in the Tanzanian SOA system. The purpose of the interviews was to (1) fill in remaining gaps in the situation analysis by qualitatively ascertaining strengths and challenges of the SOA system from the perspective of those coordinating and providing SOA care delivery and recipients of care, (2) identify champions to drive the NSOAP development and (3) raise awareness of the NSOAP. During the interviews, a balance had to be struck between engaging all relevant stakeholders and the resources and time requirements necessary to reach these stakeholders which could risk the momentum of the NSOAP development. These competing priorities were overcome by purposefully sampling across different groups of stakeholders, geographical regions and levels of care. The literature search and face-to-face situation analysis took 5 months during which in-depth, one-on-one semistructures interviews, and focus groups with over 200 stakeholders were conducted. Interviewees included surgeons, anaesthesiologists, obstetricians, non-physician SOA providers (task-sharers), nurses, policy-makers, professional and civil society organisations, patient advocacy groups, hospital managers and educators. Healthcare providers interviewed were from private and public institutions, from each of the six geographical administrative zones (which are formed of multiple regions) of Tanzania and from various healthcare levels (national, regional referral, district, health centre) to ensure balanced representation of inputs. The semistructured interviews with clinical stakeholders were accompanied by direct observation of site facilities during site visits. The majority of the interviews were carried out by members of the Harvard Team, the interview guides that were then adapted for the Tanzanian context can be found online (http://media.wix.com/ugd/346076_91d903ad9bd74869bc04502579430d5d.pdf). Following the interviews, response themes were identified using an inductive methodology, but due to a lack of available resources a full formal qualitative analysis was not undertaken. Additionally, there were extensive discussions between the different MoHCDGEC departments that would contribute to the NSOAP and its development including but not limited to the Department of Human Resource Development, Curative Services, Maternal, Child and Reproductive Health, Policy and Planning, Preventative Services and Information and Communication Technologies. The stakeholders that were interviewed were identified using a snowball technique. Although this identification technique provides an organic methodology to reach those not already in contact with the MOHCDGEC, it can be inefficient while leads are traced and may have contributed to the prolonged situation analysis phase. However, this methodology was selected as a readily available list of relevant stakeholders was not available given that this was one of the first attempts at top-down coordination of the SOA system. A benefit of the situation analysis has been to provide more cohesion to the SOA stakeholder group nationally such that consultation on the NSOAP in the future can be more efficient and this preliminary identification of stakeholders can be used as a base for iteration in the future.
Essential to the validity of the NSOAP was that as much as possible, the strategic objectives, outputs and activities within it were evidence based. As such, information from the situation analysis was synthesised into policy briefs containing all available data, which were distributed ahead of the technical workshop (described below) to structure discussion and, where possible, guide opinion with evidence during priority setting. Information had to be made concise and interpretable to the diverse group of workshop participants, many of whom were time-pressured frontline providers who would have little time to prepare and had little formal health policy experience. Some areas, such as workforce retention and supply chain management had good quality evidence for which policies were effective. However, in many areas best practice had to be extrapolated from related fields or based on expert opinion as high-quality evidence was scarce given the relatively nascent area of health policy research in surgery.
Stakeholder priority setting
The second phase of the NSOAP development was stakeholder priority setting which occurred over a 2-day national technical workshop in April 2017. Throughout the NSOAP development, the need to engage stakeholders had to be balanced against the cost of taking these vital providers, policy-makers and other professionals away from their important work. For example, in Tanzania, there are less than 20 practicing anaesthesiologists. As such, when four attended this workshop, national coverage was severely diminished. To ensure that the valuable time of workshop participants was used to maximum effect, each workshop required meticulous advanced planning with all necessary information readily available, discussion frameworks refined and a firm approach to time-keeping.
The workshop was attended by over 70 participants, including government policy-makers, clinicians (private and public), allied health professionals, professional and civil societies, non-governmental organisations (NGOs), institutions involved in the training of professionals involved in the SOA system including biomedical engineers, and private industry partners which represented urban and rural areas as well as the public and private sector, some of which are listed in online Appendix 3. The majority of workshop participants had been identified during the wider situation analysis as ‘champions’—stakeholders which when interviewed, showed high levels of engagement and expressed interest in a greater involvement with the NSOAP development.
Supplemental material
Five technical working groups were formed around the six domains of the surgical system (service delivery, infrastructure, human resources, information management, finance and governance). Each technical working group was chaired by a clinical provider to encourage a flat and open hierarchy between technical working group members. The technical working groups worked through a defined discussion framework developed by the Programme in Global Surgery and Social Change (https://www.pgssc.org/national-surgical-planning). For each domain of the NSOAP, the discussion framework guided workshop participants through an assessment of the current situation and desired situation, followed by discussion of current efforts to address any gaps between current and desired situations, possible solutions, indicators and targets, as well as responsible parties (eg, online Appendix 2). All answers and recommendations were recorded in real time by a facilitator on a communal screen to ensure transparency and that minutes accurately reflected the technical working group consensus. Each technical working group reported out to all the workshop participants. Answers to the discussion framework were then discussed by all the workshop participants until consensus of all was achieved. By the end of the workshop, priorities that would make up the strategic objectives, outputs and activities of the NSOAP had been defined.
Supplemental material
Drafting and validation
Immediately after the priority setting workshop was complete, drafting of the NSOAP began in April 2017. The first draft of the NSOAP was synthesised from the results of the priority setting by the facilitating Harvard team. The priorities from the situation analysis, interviews and workshop, were structured into strategic objectives, outputs, activities, indicators and targets for each of the six NSOAP domains (table 2). Aware of the need to avoid redundancy or incongruity, each strategic objective was checked against the map of existing policies compiled during the situation assessment to ensure alignment with current government policies (online Appendix 1).
Key strategic objectives of the National Surgical, Obstetric and Anaesthesia Plan by domain*
On completion, the first draft of the NSOAP was circulated to an NSOAP writing subgroup selected as a subgroup of the technical workshop participants. The smaller NSOAP writing subgroup of 35 participants was chosen to balance the need for wide representation with the practicalities of unifying the document into a single consensus voice. The NSOAP writing subgroup had representation from each of the original technical working groups from the priority setting workshop to ensure that the draft accurately reflected what had been discussed in each technical working group. After soliciting initial thoughts on the draft from NSOAP writing subgroup members by email, telephone and face to face, the NSOAP writing subgroup came together for a 2-day writing workshop in September 2017. Each strategic objective, output and activity in the NSOAP draft was reviewed and amended in real time until consensus was achieved. During this session, time-bound indicators and targets to measure progress against each strategic objective were defined. After the writing workshop, the agreed-upon revisions were incorporated and a final draft circulated for approval.
Costing
Following the writing workshop in September, all NSOAP activities were costed in November 2017 by the MoHCDGEC, facilitated by the Harvard team with input from a range of stakeholders from across the MoHCDGEC departments including Policy and Planning, Pharmacy, Procurement and Training. Each activity was divided into cost objects—items to which costs can be assigned—using a methodology which mirrored the national health budget (table 3). Where additional cost information was required, expert institutions and NGOs with experience in implementing surgery, anaesthesia or obstetric programme in Tanzania were approached. These included Muhimbili University of Health and Allied Sciences, Kilimanjaro Christian Medical University College and Comprehensive Community-Based Rehabilitation in Tanzania. Where national estimates were not available, international documents including the Zambian National Surgical, Obstetric and Anaesthesia Strategic Plan and other global data sources were used for reference.8
Extract from costing for NSOAP activities
Section 2: NSOAP content
The result of the work was an NSOAP, owned and endorsed by the MoHCDGEC that incorporates best practice evidence and reflects the views of the diverse stakeholders who interact with the SOA system in Tanzania. The most crucial strategic objectives, outputs and activities of the plan are summarised below and all the strategic objectives of the NSOAP are listed in table 2.
Service delivery
The organisation of the surgical service delivery system around SOA care delivery is crucial to improving the efficiency of the system. To address current inefficiencies, most activities in the service delivery domain are structured around defining the roles and responsibilities of each facility level and strengthening the referral system. Emphasis is placed on strengthening basic essential and emergency surgical care and stabilisation of patients with life-threatening conditions at lower-level facilities. District hospitals and health centres upgraded to provide Comprehensive Emergency Obstetric and Newborn Care (CEmONC) are expected to now also provide basic emergency surgical and critical care appropriate for their level (table 4). This range of services requires little extra personnel and equipment compared with those required for CEmONC. Priority is also given to strengthening comprehensive emergency and elective surgical care at zonal and regional hospitals countrywide. One zonal or regional hospital in each zone will serve as a ‘fully functioning surgical centre’ and provide basic and specialist training for the SOA workforce to address issues of workforce distribution and serve as a hub for supportive supervision to lower-level facilities. The SOA service delivery expected at each hospital level is outlined in table 4. Simultaneous strengthening of lower-level and higher-level facilities will serve to rehabilitate the referral pathway by redistributing patients to appropriate levels of care while also improving the timeliness and safety of services provided.
Service delivery expected at upgraded health centres, district hospitals and regional hospitals as stipulated in the NSOAP
Infrastructure
Previous research shows that existing health facilities are lacking in basic infrastructure required for surgical service provision. A country-wide study conducted in 2012 found that only 33% of health centres and 51% of hospitals providing surgical services in Tanzania had the appropriate personnel and equipment required for safe surgical services.14 To address these limitations, the NSOAP focuses on upgrading existing health facilities with the necessary infrastructure (including equipment and supplies) needed to provide the safe surgical services required for their level of care. All operating theatres in all health facilities are to be rehabilitated and renovated to meet the standards mandated by the MoHCDGEC.15–17 This effort aligns with the current policy outlined in One Plan II to upgrade all hospitals and 50% of health centres to provide full safe CEmONC care.18 This effort is already being supported by the MoHCDGEC as well as multiple partners such as the World Bank and other development partners. Diagnostic, laboratory, radiology, laundry and sterilisation infrastructure are also to be standardised in line with the service delivery recommended at each level, as these crucial ancillary services are often lacking.
Human resources
With a physician SOA provider density of only 0.46 per 100 000 population, compared with a target of 20 per 100 000 population, Tanzania faces an acute shortage of SOA providers to meet its population’s surgical need.19 This shortage is further compounded by an inequitable distribution of providers with a majority of SOA providers clustered in urban areas where only 30% of the population resides.20
The NSOAP aims to increase the density of physician specialist SOA providers from 0.46 per 100 000 population to 2.27 per 100 000 population by 2025. Although this does not approach the 20–40/100,000 recommended by the LCoGS, with equitable distribution, it would be sufficient to allow specialist supervision of non-specialist staff (physician and non-physician) at the district level. Achieving this will require training an additional 240 physician surgeons, 567 anaesthesiologists and 200 obstetricians. This requires an expansion of residency training which although large, was felt to be attainable by the faculty leading the training institutions. No increase in medical school matriculation is required in the context of the existing ‘surplus’ of recent medical graduates who do not have posts. These specialists can then act as trainers to increase the capacity for high-quality training in the future. The anaesthesia workforce is the most lacking with less than 20 practicing specialist anaesthesiologists in total and very limited training capacity for fully qualified assistant medical officer or nurse anaesthesia training. The plan aims to increase the density of anaesthesia providers (specialist plus non-specialist) from 0.09 per 100 000 population to 2.23 per 100 000 population by training 1100 nurse anaesthesia providers and 567 anaesthesiologists by 2025.21 To meet these targets, training is prioritised in the first phase of implementation by standardising anaesthesia curricula and ensuring that training goals reflect competencies, increasing training capacity at training institutions and ensuring sponsorship opportunities for students.22 The cost of training, salaries and retention schemes for these additional staff are included in the NSOAP costing.
The NSOAP has multiple activities to address the maldistribution of providers in Tanzania. There are incentives to encourage staffing and retention in rural regions. Additionally, the plan advocates for local specialty training through the development of regional training hubs to encourage providers to practice where they train, a factor known to improve local retention.23 Supportive supervision and continuing medical education at all levels of care are also included, as professional development opportunities have been cited as the strongest determinant of staff retention.24 Moreover, the plan advocates for the deployment of staff in functional clusters—defined as providing each unit with sufficient anaesthesia and surgical staff as well as specialist nurses in adequate numbers to allow shift and vacation relief. Adequate staffing aims to ensure safer, more efficient and consistent service delivery which, in turn will improve the referral pathway.
Information management
Data on the SOA system in Tanzania are sparse. Data availability is crucial for informed decision-making, accountability and advocacy from the facility level through to the national level. Tanzania has effective reporting mechanisms through the District Health Information Software (DHIS) within the Health Management Information System. Thus, the NSOAP aims for key surgical indicators which will be defined in a full monitoring and evaluation plan to be integrated into existing data collection and reporting mechanisms. The NSOAP commits that, at minimum, the four WDIs which relate to surgery will be reported. Other indicators specific to the Tanzanian NSOAP are yet to be defined, and their development and roll out is a strategic objective of the NSOAP. To improve feedback and action on the data collected on the SOA system, monthly surgical multidisciplinary team meetings are recommended at each care facility. These meetings would include morbidity and mortality reviews as well as a review and action plan for data collected on the facility. The NSOAP also states that it will develop the country’s institutions and process to report relevant data, such as the WDIs for surgery, on transparent national platforms (eg, DHIS) and international platforms (eg, World Bank WDI platform).
Governance
One of the key aims of the NSOAP is to improve the visibility and accountability around SOA care, which requires strong governance mechanisms. The plan defines roles and responsibilities for NSOAP representatives, as new roles within MOHCDGEC and PO-RALG, at each level of the health system from the facility to the national level. At the national level, a national coordinator at MoHCDGEC and PORALG as well as a technical working group will interact with other MoHCDGEC departments and government ministries to promote the agenda of the NSOAP and secure required resources. Representatives within the regional and council health management teams will aggregate and escalate data, ensure the coordinated inclusion of NSOAP activities into council plans and supervise NSOAP implementation.
Finance
Sustainable financing mechanisms are crucial to ensure the full implementation and attainment of targets of the first Tanzanian NSOAP. Over the 7-year period of implementation, the NSOAP will cost US$597 million adjusted for inflation and exchange rate fluctuation (table 5). This represents less than US$2 per capita per year, which is equivalent to less than 3% of the current per capita health expenditure ($52) or 1.2% of the Abuja Declaration recommended per capita health expenditure for Tanzania.25 The domains of infrastructure and workforce make up the majority of the costs (59% and 37%, respectively). 70% of the workforce expenditure is recurrent, as a reliable supply of SOA workforce needs to be trained and employed on an ongoing basis. In contrast, a high proportion of the infrastructure expenditure is capital (89%) with the remaining 11% to take into account the increased consumables (drugs, suture, equipment, reagents, etc) required when surgical volume increases, as well as the need for ongoing maintenance of infrastructure and the administration of the supply chain. The domains of service delivery, finance and governance make up a smaller proportion of the overall cost as many of the activities within these domains consist of devising new protocols and advocacy which tend to have a lower cost than infrastructure capital and salaries.
Summary of NSOAP implementation costs total 2018–2025 (USD)
Financing the NSOAP will require local, regional and national intersectoral commitments, as well as support from international partners. In order to acquire the funding detailed above, the NSOAP lays out strategies for advocating for financial support from existing and new funding sources. Given the devolved nature of government, the majority of the funding is expected to come from the inclusion of NSOAP activities in council health plans, with a minority being provided centrally by MOHCDGEC and external sources. Increased service delivery may result in increased utilisation of SOA services and therefore increased revenue from user fees which can support hospital activities. It is important that patients remain protected from impoverishing and catastrophic expenditure from such user fees. To address these risks, the NSOAP includes specific activities such as ensuring the coverage of emergency and essential SOA care in national health insurance schemes like the National Health Insurance Fund and the Community Health Fund.
Section 3: implementation
The strategy laid out in the NSOAP is designed to be ambitious, but attainable within the time, human resource, information and financial constraints of Tanzania. It contains details of new policies and a roadmap as to how they will be implemented, the parties responsible, the cost and how progress will be evaluated. While surgery and anaesthesia being relatively new to the list of national public health priorities, the NSOAP will need to attract significant domestic and international funding, which will require significant political will and commitment. For real change to occur, this commitment to improving SOA care delivery will need to continue beyond the 7-year prospects of this NSOAP and endure any political changes within government. Despite the challenges ahead, since the signing of the NSOAP significant progress has already been made. The MoHCDGEC has pledged financing from domestic and pooled international ‘basket fund’ for the training and employment of 200 3-year trained anaesthetists and a phasing out of anaesthesia practiced by non-certified providers. Additionally, the MoHCDGEC and PO-RALG are working to employ two full-time coordinators responsible for coordinating the implementation of the NSOAP which would, for the first time in Tanzania, create a department within the MoHCDGEC specifically responsible for implementation of the NSOAP and oversight of SOA care delivery. In addition to being a catalyst for implementation, these coordinators will serve as the point persons to coordinate the activities of stakeholders outside of the MoHCDGEC and PO-RALG such as professional associations and NGOs. As implementation moves forward, evaluation of the plan using rigorous implementation science methodology is required.26 27 As well as improving access to and quality of SOA service delivery in Tanzania, a crucial aim of this plan is to generate new evidence as to what policies within the SOA system work to improve outcomes for patients as well as what is needed to implement them successfully. This will serve to iterate and improve the strategies to improve SOA care delivery worldwide as more countries commit to the creation of NSOAPs. This will also serve to inform and improve the next NSOAP in Tanzania which would take the country beyond 2025. Lessons learnt from the development of the NSOAP in Tanzania are summarised in Box 2.
Lessons learnt
The directive of a high ranking, influential, member of the Ministry of Health, preferably the Minister of Health (MOH), is crucial to ensuring the process is owned by the MOH. The MOH receives many external recommendations from different agencies, only through the process being internally driven will the chances of adoption be high.
Initial stakeholder engagement must weigh up the benefits of getting more people on board with the time and financial resources required to do so. Purposeful sampling to ensure diverse cross-sectional representation can be an efficient way to do this.
Engaging early and widely across many departments within the Ministry of Health means there is greater support for the plan’s approval once drafted. Early engagement with the Ministry of Finance, although not possible in this example, is likely to improve budget allocation for implementation.
Throughout the development process, a cornerstone philosophy must be that stakeholders time is extremely valuable and National Surgical, Obstetric and Anesthesia Plan (NSOAP) development is another demand on their time. This should be recognised, and meticulous planning for each step is required to ensure their time is used to maximum efficiency.
During situational analysis, a thorough review of existing materials especially existing reports, data and publications can avoid resource-intensive duplication of efforts through repetitive data collection.
A thorough mapping of existing policies that may influence the NSOAP is crucial to avoid clashing or overlapping policies and to gain a deep understanding of what may be driving the existing priorities of stakeholders.
The process can easily lose momentum and interest of stakeholders. Compromises on the depth and breadth in the NSOAP must be made to ensure the process is actually completed. These compromises are aided by a thorough understanding of what policies already exist therefore do not require repetition.
Information from the situational analysis should be processed into an easy to follow and engaging format of realistic length for stakeholders to read ahead of any priority setting. Lengthy documents are unlikely to be read. This allows for this information to be leveraged to inform opinion and decision-making as opposed to occurring as a parallel process.
It is crucial for the validity of the process that the group responsible for the initial drafting use only consensus decisions from the priority setting and do not unilaterally add or withdraw information from draft at this stage.
The plan should be advised by stakeholders but written by policy-makers to ensure it aligns with current policy frameworks and costing and implementation methodologies are consistent with current norm. This also helps ensure the plan is not overly ambitious becoming a ‘wish-list’ as opposed to an implementable strategy.
All potential sources of funding in quality and quantity should be considered before embarking on the NSOAP development process and a plan for mobilising key financing stakeholders developed at the start of the development process.
A large proportion of the activities of the NSOAP do not require additional funding for material costs but do require dedicated staff to arrange and advocate for the recommendations. As such one the priority areas for funding for NSOAP should be full-time staff within the MOH dedicated to NSOAP implementation as this may be the most cost-effective spend in the short to medium term. These staff can then continue to advocate for allocation of additional resources for other activities. Ideally, this staff should be brought on at the beginning of the NSOAP development process and be central to it, although this may be challenging as without an NSOAP there is unlikely to be funding for this position.
Conclusion
Achieving UHC 2030 and the Sustainable Development Goals will not be possible without addressing the burden of disease resulting from surgically treatable conditions.28 Through the development and launch of its first NSOAP, Tanzania has taken an essential step towards improving surgical, anaesthesia and obstetric service delivery. The NSOAP ensures the essential domains of the SOA system are addressed simultaneously to improve efficiency, coordination and ultimately impact. The NSOAP also provides an effective platform to advocate for additional resources for SOA care. The successful implementation of the priorities of this ambitious plan will rely on effective intersectoral collaboration between public and private efforts in Tanzania as well as support from international development partners. Ultimately, the NSOAP will only be successful if it achieves meaningful changes in outcomes for patients with conditions amenable to surgery, anaesthesia and obstetric care.
Footnotes
IC and DJ are joint first authors.
JM and MU are joint senior authors.
Handling editor Seye Abimbola
Contributors IC: Conceived the paper, led design and execution of process and paper, wrote manuscript, edited DJ: Conceived the paper, led design and execution of process and paper, wrote manuscript, edited JD: Executed the study, revised manuscript. SM: Strategic advice throughout the design and execution of the process, reviewed manuscript. KN: Research and execution of study, reviewed paper KI: Research and execution of study, reviewed paper LA: Led design and execution of the process, reviewed paper EL: Led design and execution of the process, reviewed paper BD: Led design and execution of the process, reviewed paper SM: Led design and execution of the process, reviewed paper BN: Design and execution of the process, reviewed paper NK: Design and execution of the process, reviewed paper AH: Strategic advice throughout the design and execution of the process, reviewed manuscript EM: Strategic advice throughout the design and execution of the process, reviewed manuscript SK: Strategic advice throughout the design and execution of the process, reviewed manuscript PM: Strategic advice throughout the design and execution of the process, reviewed manuscript CR: Strategic advice throughout the design and execution of the process, reviewed manuscript AV: Strategic advice throughout the design and execution of the process, reviewed manuscript DB: Strategic advice throughout the design and execution of the process, reviewed manuscript MS: Conceived paper, Strategic advice throughout the design and execution of the process, reviewed manuscript JM: Conceived project and paper, Strategic advice throughout the design and execution of the process, reviewed manuscript MU: Led project and paper, led execution of the project, reviewed manuscript.
Funding Funding for the development of the NSOAP was provided by the GE Foundation through the Safe Surgery 2020 (SS2020) initiative.
Competing interests None declared.
Patient consent for publication Not Required
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.