Article Text

Abstract
Background and methodology The Standard Days Method® (SDM) is a fertility awareness-based method of family planning that helps users to identify the fertile days of the reproductive cycle (Days 8–19). To prevent pregnancy users avoid unprotected sexual intercourse during these days. A cross-sectional community-based study was conducted from December 2007 to June 2008 in four operational areas of Pathfinder International Ethiopia. A total of 184 SDM users were included in the study. Quantitative and qualitative methods of data collection were used. The aim of the study was to examine the experience of introducing the SDM at community level in Ethiopia.
Results Of the 184 participants, 80.4% were still using the SDM at the time of the survey, with 35% having used it for between 6 and 12 months, while 42% had used it for more than a year. The majority (83%) knew that a woman is most likely to conceive halfway through her menstrual cycle, and nearly 91% correctly said that the SDM does not confer protection from sexually transmitted infections/AIDS. A substantial majority (75%) had correctly identified what each colour-coded bead represents in the CycleBeads®, and an aggregate of 90.5% of women practised all the elements of correct use.
Discussion and conclusions This study demonstrates the importance of the SDM in increasing the availability and accessibility of family planning, and the potential to improve family planning method choice and method mix by expanding use of the SDM.
Statistics from Altmetric.com
Introduction
Ethiopia is the second most populous country in Africa1 with high maternal mortality ratio (673 per 100 000 live births). Though there has been a decline in fertility from 6.4 births per woman in 1990 to 5.4 births in 2005, this rate is nevertheless still very high. The 2005 Ethiopian Demographic and Health Survey (EDHS) suggests that while 88% of currently married women and 93% of currently married men were aware of at least one method of contraception, only 15% of married women were using a contraceptive method. The contraceptive prevalence was more than four times higher in urban (47%) than in rural (11%) areas. Modern contraceptive methods were more widely practised than traditional methods, with 14% of currently married women using a modern method, and 1% using a traditional method. The most popular modern method was the injectable followed by oral contraceptive pills. The unmet need for family planning was calculated to be 34%, with 20% for spacing and 14% for limiting.2
Key message points
▶ The Standard Days Method® (SDM) has great potential for increasing the availability and accessibility of family planning in Ethiopia.
▶ The vast majority of women understood the elements for the correct use of the SDM method, and were willing to continue using this method.
▶ The SDM is an important addition to the method mix of family planning method choice in Ethiopia.
Knowledge about fertility and reproductive physiology is very low in Ethiopia. Only 11% of women and 8% of men could identify the middle of the menstrual cycle as the time women are most likely to become pregnant.2 The low level of knowledge about the fertile period is an important factor accounting for unplanned pregnancies.2 A way of averting unplanned pregnancies resulting from poor knowledge about reproductive physiology and fertility can be offered by fertility awareness-based (FAB) methods of family planning.3 FAB methods of family planning provide women with simple, clear instructions for identifying the fertile days in their cycle.4
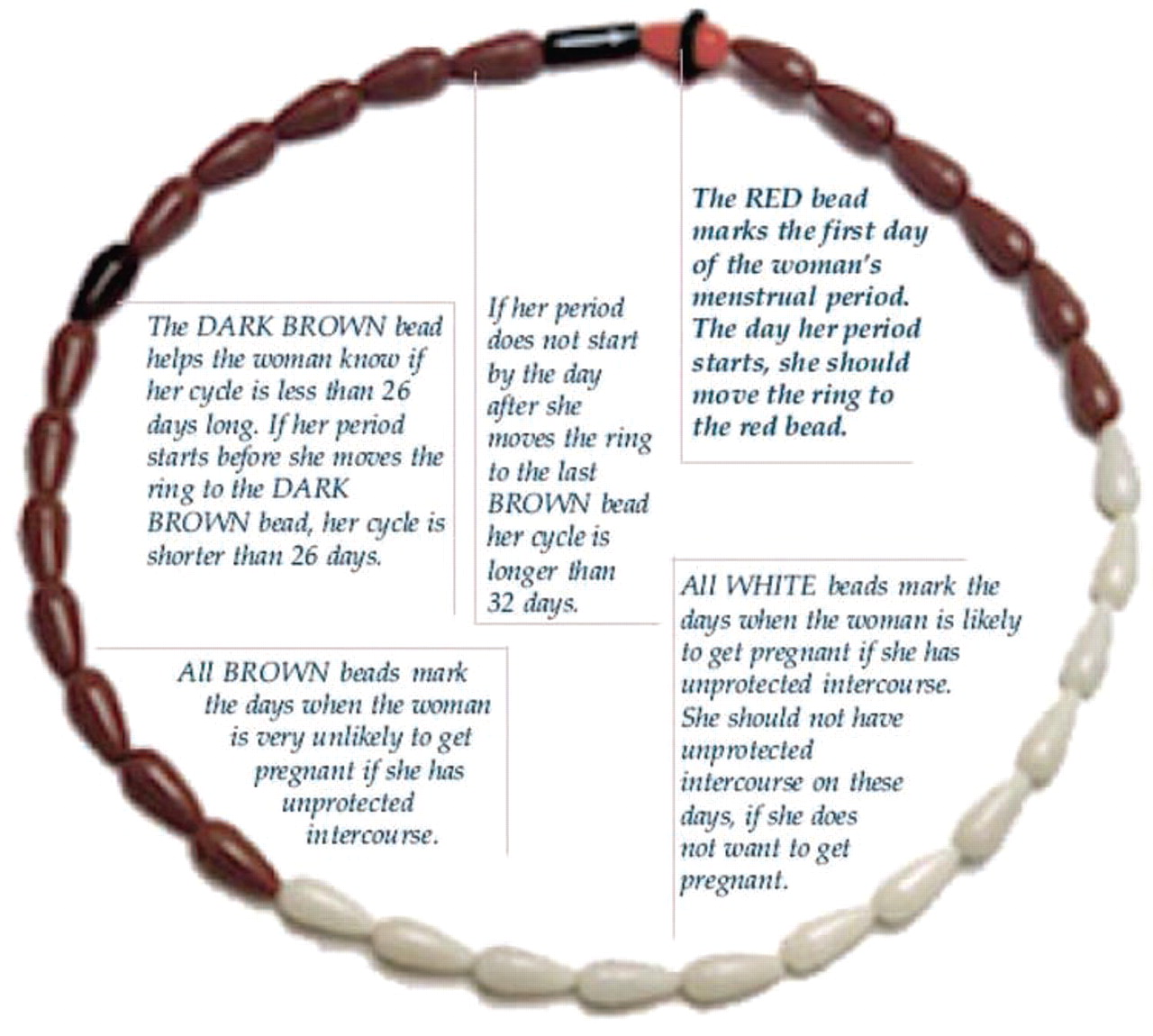
The Standard Days Method® (SDM) is a simple, effective FAB method of family planning. It was developed and tested by the Institute for Reproductive Health, Georgetown University, Washington, DC, USA. It identifies Days 8–19 (inclusive) of the menstrual cycle as the fertile window for all users in all cycles. The target group is women with menstrual cycles that usually range from 26 to 32 days who are willing to avoid unprotected sexual intercourse (UPSI) during the fertile days. Women should also be advised to choose another method if they have a second cycle outside the 26–32-day range in a year.3 CycleBeads® (Cycle Technologies, Washington, DC, USA), a colour-coded string of beads, is a visual tool that helps women learn and use the SDM by helping them track their cycle days, identify when the woman is fertile and monitor her cycle length.5 Figure 1 illustrates how the CycleBeads work.5 A prospective, multicentre efficacy trial of SDM showed a cumulative probability of pregnancy of 4.75% (95% CI 2.33–7.11) over 13 cycles of correct use of the method, and 11.96% probability of pregnancy with typical use.6

Illustration of how the CycleBeads® work. Image reproduced by kind permission of the Institute for Reproductive Health, Georgetown University, Washington, DC, USA5
The introduction of the SDM in family planning programmes is an important addition to the family planning method mix that could help to increase contraceptive prevalence and reduce the level of unmet need, promote informed choice by expanding family planning method options, and contribute to increased male involvement in the range of reproductive health decisions.7 Besides this, the SDM could also help in securing contraceptive supplies by closing the family planning funding gap.7 ,8
The SDM was introduced in Ethiopia into community-based service delivery setting in 2004 by Pathfinder International Ethiopia with the assistance of the United States Agency for International Development, and in collaboration with five implementing partner organisations of Pathfinder International Ethiopia (Relief Society of Tigray, African Humanitarian Aid Organization, Medan Act Project, Abebech Gobena Project and Oromiya Development Association). Pathfinder International Ethiopia, a non-governmental organisation working on expanding access to and use of family planning/reproductive health services, took the initiative and decided to introduce the SDM into its community-based programme in an effort to increase method mix and improve method choices for clients. The sites in which the SDM was routinely offered were Dilla town, Dendi woreda, Adigrat town, Wolaita zone and Denbidolo town. Though data on the contraceptive prevalence rate (CPR) of each of the service sites were not available, the CPR of the regions where the service sites were located were 11.9% (Adigrat town), 16.5% (Dilla town and Wolaita zone) and 13.6% (Dendi woreda and Denbidolo town).2 Initially 17 health professionals (i.e. medical doctors, health officers and nurses) were provided with training for trainers on the SDM followed by a roll out training for 129 community-based reproductive health agents (CBRHAs) from 2004 to 2006. The CBRHAs provide family planning/reproductive health information/services at the community level and maintain referral linkages to fixed government health facilities. The agents, with the support of the implementing partner organisations of Pathfinder International Ethiopia, offer information and services through community interactions including house-to-house visits, counselling at religious gatherings, festivals and other community events, and market place discussions. Information, education, communication (IEC) and behavioural change communication (BCC) activities (IEC/BCC) such as health education, posters and brochure distribution, and educational messages were used to raise awareness of the SDM and other family planning methods. The CBRHAs offer the SDM, oral contraceptive pills and barrier methods as part of a package of family planning methods and services, and refer clients to the health facilities for other methods of contraception.
According to the World Health Organization, the introduction of contraceptive methods should focus not on a technology-driven approach, but rather on how a new method responds to peoples' needs and rights, as well as on how it enhances overall quality of care and broadens the options available to clients.9 This study was carried out in order to examine users' perspectives and needs regarding SDM introduction in community service delivery settings. It was envisaged that the findings from this study would contribute key information for policymakers/programme managers to help determine the best way of integrating quality SDM services widely into the national family planning programme.
The primary aim of this study was to assess clients' knowledge about the SDM, and to measure the correct use of this contraceptive method among clients who chose to use it. The secondary aim was to examine the reasons for discontinuing use of the SDM, and to assess clients' intentions regarding the continued use of this method.
Methods
A cross-sectional community-based household study was conducted from December 2007 to June 2008 in four operational areas of Pathfinder International Ethiopia.
Respondents were enrolled from four purposively selected districts in Dilla town (Medan Act project area), Dendi Woreda (Abebech Gobena project area), Wolaita zone (African Humanitarian Aid project area) and Adigrat town (Relief and Rehabilitation Society of Tigray project area) in which the SDM was routinely offered.
The study population comprised women aged 15–49 years who chose to use the SDM for family planning. SDM clients were identified and referred to primary data collectors through CBRHAs (SDM providers) since all clients receive regular home visits by their respective CBRHAs. Quantitative and qualitative methods of data collection were employed. For the quantitative household survey, SDM clients were interviewed by trained female data collectors (who had completed a minimum of 12th grade education) using a pretested and structured questionnaire. The questionnaire was first prepared in English and then translated into Amharic, Tigrigna and Afanna Oromo (local languages) and retranslated back to English to check for consistency. The questionnaire comprised sociodemographic characteristics, management of fertile days, knowledge, and correct use of the SDM. The SDM clients who participated in pretesting the questionnaire and women who were sick and not available in their residential area during the time of survey were excluded from the study. For the qualitative survey, a purposive sampling technique was used to select participants for the in-depth interviews. In-depth interviews were conducted with eight CBRHAs and 11 male partners of SDM users. The in-depth interviews were conducted by the principal investigator. To obtain comprehensive information, participants were selected from four study sites. Duration of SDM use (at least 18 months), willingness to participate in the study, and being easily accessible in their residence at the time of data collection were taken as criteria to recruit male partners for interview. The main reason for recruiting male partners of women who used the SDM at least for 18 months was to discern and learn lessons about their involvement in the method use, experiences, and the difficulties encountered during their lengthy experience of method use.
Informed consent was obtained from the study participants after they were briefed about the objectives and procedures of the research. The questionnaires were anonymous and confidentiality was strictly maintained.
Data entry and analysis were conducted using Statistical Package for the Social Sciences (SPSS) Version 13.0 for Windows (IBM, New York, NY, USA). Odds ratios (ORs) with 95% confidence intervals (CIs) were used to measure the degree of association between correct use of the SDM and associated factors.The in-depth interviews were transcribed in Amharic and the transcript was then translated to English for analysis. The qualitative data were categorised using key thematic areas and the data were interpreted and presented as verbatim notes.
Results
A total of 184 SDM users were interviewed. Table 1 shows the sociodemographic characteristics of the study population. The mean and median ages were 29.47 (SD ± 6.05 years) and 30 years, respectively. The majority of the study subjects were Orthodox Christians (76.6%), married (93.5%), attended primary school (52.2%), housewife by occupation (40.8%), and had children (96.2%), with a mean of 3.2 children per woman. On average the study subjects had used the SDM for 13.8 months. Seventy-seven women (42%) had practised the SDM for more than 1 year, while 64 (35%) had used the method for between 6 months and 1 year.
Sociodemographic characteristics of Standard Days Method® (SDM) clients, Ethiopia, 2008 (n=184)
Contraceptive use prior to SDM adoption
One hundred and forty-seven (80%) study participants had ever practised some form of contraception before adopting the SDM, whereas 37 (20%) had never used any method of contraception previously. Of those who had practised contraception in the past, oral contraceptives (n=98, 66.7%) were the most common method, followed by the Depo-Provera® injectable (n=86, 58.5%), implants (n=10, 5.4%), lactational amenorrhea method (n=5, 2.7%), rhythm method (n=5, 2.7%), intrauterine device (IUD) (n=4, 2.1%) and withdrawal method (n=1, 0.7%).
Reasons for choosing the SDM
The most common reasons for choosing the SDM were absence of health effects/side effects, in 129 (70.1%) cases, followed by fear of side effects, particularly of hormonal contraceptives (n=99, 53.8%), and ease of use (n=9, 4.9%). Additional reasons were the fact that it is available without cost to the individual (n=5, 2.7%) and because it is a natural method (n=5, 2.7%). Although FAB methods are frequently associated with religious beliefs, only one woman gave this response as a reason for selecting the SDM.
SDM discontinuation
One hundred and forty-eight (80.4%) of the clients were using the SDM to avoid pregnancy, while 36 (19.6%) had discontinued using the method at the time of the interview. We interviewed these 36 women in order to ascertain their reasons for discontinuation. Ten had to stop using the method because they had two menstrual cycles that fell outside the 26–32-day range within a year. Seven women discontinued the method because they did not trust it. Six women wanted to become pregnant, and four were widowed/divorced (Table 2).
Reasons for discontinuing the Standard Days Method® (SDM), Ethiopia (n=36)
The results given in the following sections are based on the 148 participants who were still using the SDM at the time of the interview (and not on the total number of clients who had chosen to use SDM).
Method switching after SDM discontinuation
Most (20) of the women who had stopped using the method were using other contraceptive methods, while 11 had not been practising any form of family planning during the survey. The majority of them were in fact not in need of contraception at the time of the survey. Of the women who had switched to other methods of contraception, 11 chose the Depo-Provera injectable, five preferred implants, three were taking the oral contraceptive pill, and only one had switched to the IUD.
Management of the 12 fertile days
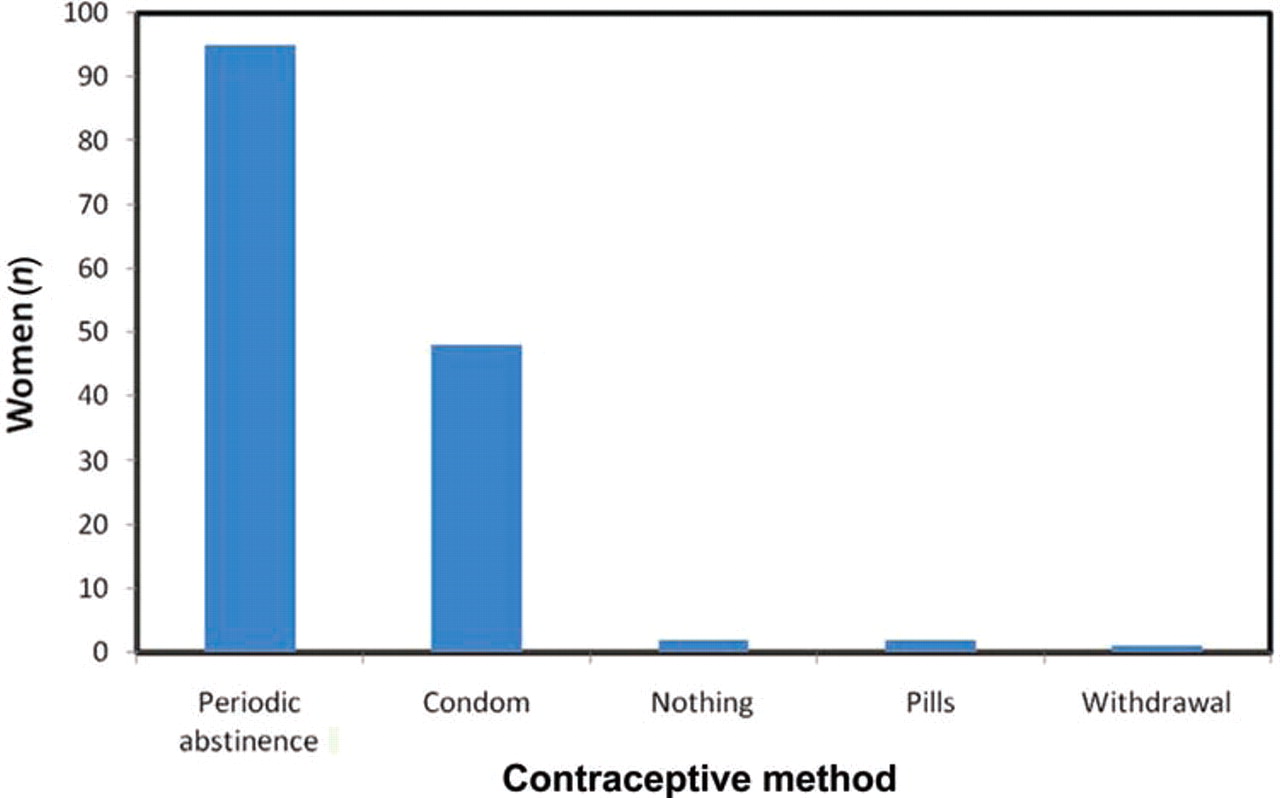
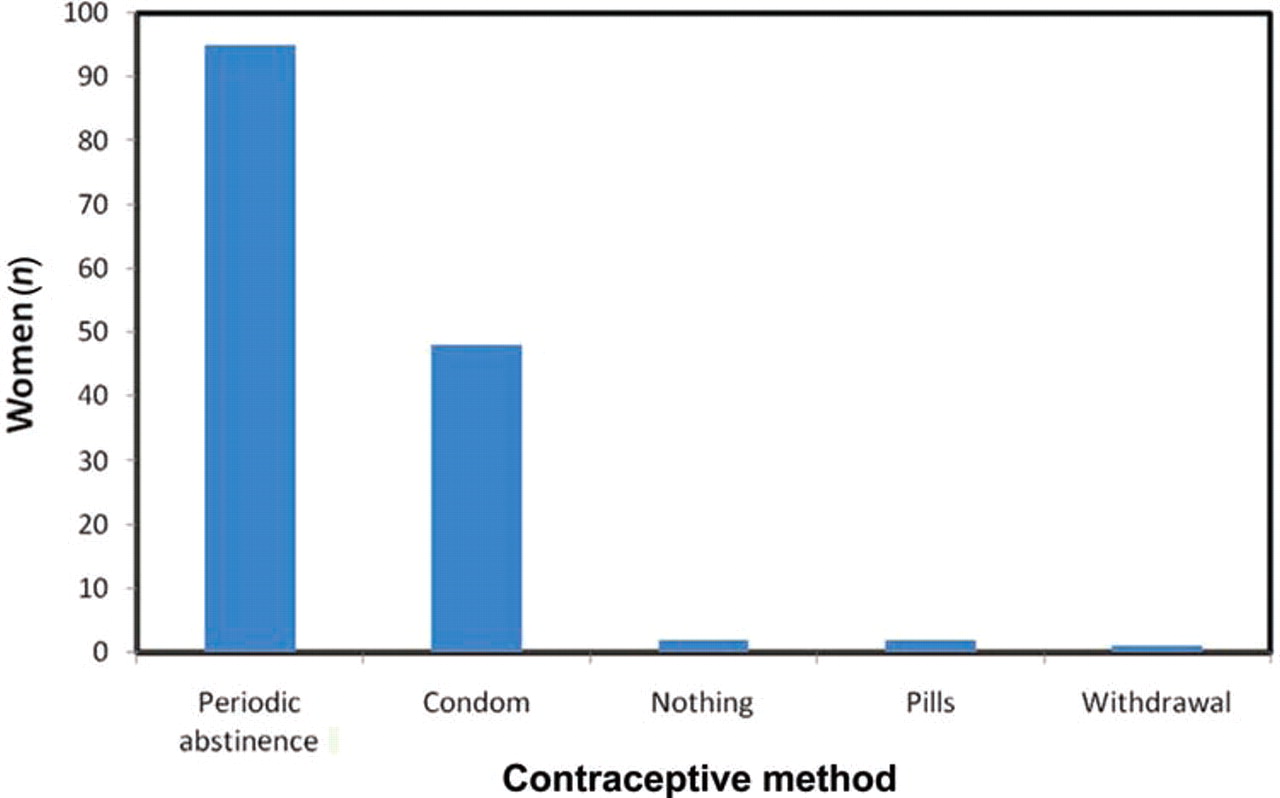
When clients were interviewed about their strategies to manage their fertile days, 95 (64.2%) practised periodic abstinence, 48 (32.4%) used condoms, two (1.4%) did nothing to avoid pregnancy, and one (0.7%) practised the withdrawal method during the fertile days. However, two were taking oral contraceptive pills during the fertile window (Figure 2).
{kind=link}
{kind=link}
Strategies used by the study participants to manage the fertile days, Ethiopia, 2008 (n=148).
Forty eight (32.4%) of the women reported that there were occasions when their partners insisted on having UPSI while they were on fertile days, whereas the majority (n=100, 67.6%) had no such experiences.
Almost half (n=73, 49.3%) the clients reported that their partners and/or they had ever consumed alcohol during the fertile days. Of these women, six (8.2%) indicated that periodic abstinence or condom use had become difficult on these days. The remaining 66 (90.4%) women reported that alcohol drinking had no effect on managing the fertile days, while one gave no response for this question.
Intention of continuing or discontinuing the SDM
In the survey group, 146 (98.7%) and 140 (94.6%) women intended to continue using the method for the next 3 months and 1 year, respectively. Likewise, equal numbers of women indicated that their partners agreed to this. Two (1.4%) clients did not intend continuing to use the method for the next 3 months, due to their desire for a pregnancy. Similarly, of the six (4.1%) women who did not intend to continue for another year, five gave a desire to be pregnant as their reason, while one wanted to use a permanent contraceptive.
Knowledge and correct use of the SDM
Based on the interview about their knowledge of the fertile days, close to 83% (122/148) of the women correctly reported that a woman is most likely to conceive halfway through her menstrual cycle. Nearly 91% correctly said that SDM does not confer protection from sexually transmitted infections (STIs)/HIV/AIDS.
When women were interviewed about their knowledge of the colour-coded beads, 122 (82%) correctly reported that brown beads represent days on which a woman is very unlikely to get pregnant. One hundred and thirty-one (89%) women correctly reported that white beads represent days on which a woman can get pregnant. Most (n=135, 91 %) of the women also correctly indicated that a red bead represents a day when menstrual bleeding begins. Only 57 (39%) women correctly reported that a dark brown bead is useful in determining whether the menstrual cycle is shorter than 26 days (Table 3).
Knowledge of Standard Days Method® (SDM) clients about the method, Ethiopia, 2008 (n=148)
This survey also measured the correct use of the SDM. Correct use of the method was measured by placement of the ring on the red bead on the first day of menses, moving the ring along one bead every day, and avoiding UPSI on the fertile days. One hundred and thirty-five (91%) women correctly placed the black ring on the red bead when their menses begin. However, nine (6.7%) and one incorrectly placed the black ring on the brown and white beads when their menses began, respectively. Three (2%) women reported that they did not know on which bead the black ring must be placed when their menses begin. Almost all the women did not have a calendar (supplied by the provider) on which to mark the first day of menses. One hundred and thirty-eight (93%) women reported that they moved the black ring along one bead every day, even on the days of menstruation. Only 10 (6.7%) indicated they did not move the black ring every day. Of the 138 women who moved the black ring along one bead every day, a substantial majority (97%) found it easy to remember to move the black ring every day. One hundred and thirty-four (90%) women had never practised UPSI when the black ring was placed on the white beads or fertile days. However, 10% had UPSI on the fertile days. An aggregate of 90.5% of women practised all the elements of correct use of the SDM (Table 4).
Distribution of Standard Days Method® (SDM) clients by correct use of the method, Ethiopia, 2008 (n=148)
Women's opinion on male partners' involvement
Based on the results of the interviews, almost three quarters (76.4%) of the study participants reported that their male partners were involved in SDM use. Thirty-five (23.7%) revealed that their partners had no involvement in SDM use. Of the 113 women whose partners were involved in SDM use, 52 (46%) men were involved by reminding their partners to move the black ring on the CycleBeads, 30 (26.6%) reminded their partners about fertile days and 28 (24.8%) of the male partners were responsible for moving the black ring every day. Ten (8.9%) of the male partners co-operated by avoiding UPSI on the fertile days, while two (1.8%) registered the date on which menses began. One hundred and thirty-seven (92.6%) of the women reported that their male partners found managing fertile days easy. The remaining 11 (7.4%) reported that their husbands experienced difficulty in managing fertile days.
Male partners' views on use of SDM
The male partners said that they decided to use the SDM because it is a natural family planning method, and has no health risks/side effects.
“When we were informed about the existence of SDM as a family planning method choice by our Keble's CBRHA, we immediately decided to use it because SDM is a natural family planning method, no hormone [medicine] to take, and doesn't contradict with our religion.” (31-year-old priest farmer participant, Adigrat town)
“My wife suffered from the side effects of pills and injectable, so we chose SDM to space our births.” (32-year-old participant, Wolaita zone)
Some of the men also explained their decision to use the method by saying that the SDM is simple to learn, easy to use, and it doesn't require calculation as compared to other natural family planning methods like the rhythm (calendar) method.
“My wife and I used to practise calendar [rhythm] method to plan our births. After the introduction of SDM as a family planning method choice, we chose SDM because SDM is simple to learn and easy to use as compared to rhythm [calendar] method.” (22-year-old male partner, Dilla town)
Most of the male partners reported that they had never encountered any difficulty in the use of the SDM. However, a few mentioned that their wives experienced irregular menstrual cycles.
“We have never encountered any problem in the use of SDM because both of us are happy and interested to use the method.” (34-year-old participant, Dilla town)
“The problem that we encountered in our two years of SDM use was irregularity of my wife's menstrual cycle.” (24-year-old male partner, Dendi Woreda)
The majority of male partners used periodic abstinence to manage the 12 fertile days. However, a few reported condom use during the white bead days.
“We rely on abstinence during the twelve white bead days.” (28-year-old participant, Dendi Woreda)
“During the white bead days, we use condoms to avoid unplanned pregnancy.” (34-year-old participant, Dilla town)
In addition, most of them found managing fertile days easy. Very few, however, found it difficult to abstain or use condoms during the fertile days.
“We have large family and numerous economic problems, so it is easy and better to abstain during dangerous [fertile] days rather than worsening our problems.” (24-year-old male partner, Dendi Woreda)
“For me, it is easy to manage the white bead days. If I want to have sexual intercourse, I can use a condom.” (36-year-old participant, Adigrat town)
Most of the male partners reported that they consumed alcohol during the fertile days but that this had no effect on the management of the fertile days.
“When I drank alcohol during the white bead days, we agree to sleep in separate beds to keep ourselves from having unprotected sexual intercourse. Sometimes, I forget the dangerous days [fertile days] after having some alcohol but my wife informs me not to have unprotected sexual intercourse by reminding me the dangerous days [white bead days].” (44-year-old male partner, Dendi Woreda)
The male partners are involved with SDM use by reminding their wives to move the black ring, avoiding UPSI during fertile days, moving the black ring one bead every day, and registering the date on which their wives' menses began.
“I participate by reminding my wife to move the black ring.” (40-year-old male partner, Adigrat town)
“I participate in moving the black ring of CycleBeads every day and my wife only informs me the date her menses begins so that I register it in my note book.” (28-year-old farmer, Dendi Woreda)
Providers' attitude and experience of the SDM
Providers reported that clients are very much interested in the method because the SDM has no health effects/side effects, is simple to learn, and easy to use. It also improves male partners' involvement with the method, and couples' communication regarding sexuality.
“My clients chose the method because they were complaining about the side effects of oral contraceptives and injectable. When I informed them about the introduction of the new family planning method, they became interested to use the SDM.” (36-year-old provider, Adigrat town)
“During counselling of clients, I gave more attention for counselling of male partners because if male partners are convinced and involved in the method, couples are more likely to use the method correctly and I make sure that the couples have mutual understanding to use the method before providing the CycleBeads to my clients.” (33-year-old provider, Dendi Woreda)
The providers had encountered difficulty in offering the SDM as a family planning option. The counselling of clients takes too long and requires continuous follow-up, especially during the first 3 months until the clients fully understand the method. Distrust of the method by some clients, unavailability of a provider-supplied calendar on which to mark the first day of menses, breakage of the black ring, and the uncooperativeness of a few of the male partners in managing the fertile days were the other factors posing problems in respect of offering the method as a family planning method option for clients.
“Clients do not understand the method easily. For me, it takes two to three days to counsel a client and needs repeated visits until couples fully understand the method.” (32-year-old provider, Adigrat town)
“I know very well about the importance of provider calendar during the training but I do not have any provider calendars to give to my clients.” (38-year-old provider, Dendi Woreda)
All providers expressed their interest in continuing to offer the SDM as a family planning method option. The providers felt that the SDM enabled them to expand their family planning method choices. They recommended that the method should also be offered in other parts of the country.
“I am very much interested in continuing to offer SDM as a family planning option for clients because it increases my family planning method choices, especially for clients who are dissatisfied with their previous hormonal family planning method. As a result, I recommend SDM to be offered in other parts of the country.” (32-year-old provider, Adigrat town)
We interviewed providers about the eligibility criteria of the SDM; however, some of the providers did not fully understand the SDM eligibility criteria.
The providers recommended the need for refresher training on SDM counselling and provision because their previous training on the method was 3 years ago.
“I trained on how to counsel clients and offer SDM three years ago, so I need to have refresher training. This will improve my competence and motivate me to do much better than what I am doing.” (42-year-old provider, Wolaita zone)
Despite some providers complaining that method counselling takes a long time and the need for continuous follow-up, providers found it easy to provide the SDM, felt confident in responding to clients' queries, and were interested in continuing to offer the method.
Discussion and conclusions
This study examined the introduction of the SDM into community-based service delivery settings in Ethiopia. The findings of this study indicate that the SDM has great potential to increase the availability and accessibility of family planning services in the community.
In nine out of the 14 study sites, most SDM users had reported previous use of family planning.10 In the present study, a substantial majority (80%) of SDM users had practised some form of contraception in the past before adopting the SDM. Conversely, most (129, 70.1%) of the clients and 99 (53.8%) cited “have no health/side effects” and “fear of perceived side effects of hormonal family planning methods” as the reason for adopting the SDM, respectively. This finding is similar to the findings of the multisite operational study,10 and a study conducted in India.11 These studies suggest that the SDM tends to be perceived by couples as being an effective, easy, low/no cost and safe alternative family planning option for those dissatisfied with their previous family planning method(s) and those who are concerned about the side effects of other contraceptive methods. Contrary to the above findings, studies conducted in Rwanda,12 and in four of the study sites of the multisite operational research on the SDM (Benin, El Salvador, Honduras and India),10 demonstrated that the majority of the study participants had never used any contraceptive methods before adopting the SDM. In the present study only 20% of the study participants had not reported previous use of family planning methods. This result also suggests that the SDM serves to add new family planning users to the overall contraceptive prevalence.
We found that 148 (80.4%) clients were still using the method, while 36 (19.6%) had discontinued use at the time of the survey. Of those 36, 10 reported having experienced two or more menstrual cycles that fell outside the 26–32-day range. This finding is consistent with studies of SDM efficacy in Bolivia, Peru and The Philippines,6 Rwanda12 and Istanbul.13 A stringent, ongoing menstrual cycle monitoring protocol must be followed until the woman has two cycles that fall outside the 26–32-day range within a 1-year timeframe. It also reduces the probability that women with very irregular cycles will continue using the method, and therefore improves method efficacy.14 Twenty (20/36) women who had stopped using the method had switched to other methods of contraception. This finding suggests that it is important that users understand the importance of cycle length and that programmes provide a wide range of family planning method options to meet clients' needs. Two women became pregnant while using the SDM because they had UPSI during their fertile days.
The majority (94.6%) of the 148 women who were still using the SDM at the time of the survey intended continuing to use the method for the next 12 months, a finding comparable to that of the study conducted in Rwanda.12 This implies that these women were greatly satisfied with, and had an interest in, their current family planning method.
Periodic abstinence (64.2%) and condom use (32.4%) were the usual methods used by the women to manage the fertile days. Similarly, the multisite operational study on the SDM10 and a study conducted in Rwanda12 revealed that periodic abstinence and condom use were the leading strategies employed to manage the fertile days. However, two clients had taken oral contraceptive pills during their fertile days. This might have occurred due to poor counselling of clients, lack of follow up, or male partners failing to participate in the method use. Effective counselling of couples on strategies for handling the fertile days can help them to manage those days effectively and improve correct use of the SDM.
Nearly half the women reported they and/or their partners had ever consumed alcohol during the fertile days. Of these women, six (8.2%) had encountered difficulties in managing the fertile days. This finding suggests that providers should place sufficient emphasis on the screening of clients for issues such as alcohol consumption that may undermine the successful use of the SDM, and indicates that thorough counselling should be offered to potential SDM users in order to address these issues.
It is interesting to note that close to 83% of the study participants reported that a woman is most likely to conceive halfway through her menstrual cycle, a finding much higher than was noted in the 2005 EDHS.2 This difference is due to the fact that SDM use helps women to identify their fertile and infertile days.5 ,6 As regards their knowledge about the colour-coded beads, a substantial majority (75%) had correctly stated what each bead represents in relation to identifying the fertile and infertile days. However, only 39% of participants knew what the dark brown bead represented in terms of fertility. This suggests that providers need to ensure that clients are well versed in the use of the CycleBeads as this is crucial for correct method use. Nearly 91% of participants knew that the SDM does not confer protection from STIs/HIV/AIDS. However, five participants wrongly believed that the SDM offers protection from STIs/HIV/AIDS, while nine said they didn't know. It is known that counselling for the SDM includes screening clients for the risk of STI/HIV infection. However, in addition to this screening process, information from providers should stress the fact that SDM does not confer protection from STIs/HIV/AIDS.
An aggregate of 90.5% of women practised all the elements of correct use of the SDM, a finding comparable with a study conducted in India.11 Despite a high level of correct use of the method, almost none of the women had been provided with a calendar on which to mark the first day of their menstrual cycle. This issue was a very sensitive one, and required urgent action from the programme offering the SDM. Following the survey this problem was totally rectified. In the multisite efficacy studies of SDM and 2-day methods, 23% of the study participants had UPSI on a fertile day in at least one cycle.4 ,15 In the present study, only 10% had ever practised UPSI on a fertile day in at least one cycle. The providers should not only teach clients the correct use of the SDM, but also assist them in learning negotiating skills. Furthermore, the providers should also make sure that the women understand the consequences of having UPSI on fertile days and involve men in the counselling also.
An important finding was that men were actively involved in SDM use by reminding their wives to move the black ring, avoiding UPSI during fertile days, moving the black ring every day, and noting the date on which their wife's menses began. Introduction of SDM into family planning programmes is likely to contribute to increased male involvement in a range of reproductive health decisions.7 ,16
Community-based reproductive health agents showed great satisfaction and interest in offering the SDM as a family planning option. This suggests that community-based providers can provide the SDM effectively with adequate training and supervision. However, some of the providers had complained that the SDM necessitated time-consuming counselling sessions. Studies conducted in India (SDM 10 minutes vs Pill 8 minutes),17 Rwanda (SDM 44 minutes vs Pill 38 minutes)18 and Peru (SDM 23 minutes vs Pill 15 minutes)19 demonstrated that the SDM can be offered with a similar length counselling session as required for the oral contraceptive pill. The amount of time needed to counsel new SDM users typically did not exceed what is generally allocated in respect of new family planning consultations.10 Some of the providers themselves had not mastered the eligibility criteria for the SDM and they also recommended the need for refresher training. Refresher training and supportive supervision is essential for the sustained capacity of SDM providers, thereby ensuring the quality of services.20 The programme offering the SDM needs to provide refresher training for the providers in order to improve their knowledge about the method.
The present study has some limitations. Longitudinal study design (follow-up interviews) could have provided in-depth knowledge for computing pregnancy rates using life-table analysis. Another limitation is that only recruitment of male partners of women who have used the method for 18 months or more for in-depth interviews might have introduced bias.
Based on the results from the study districts, stakeholders including Amhara and Oromo development associations have introduced the SDM widely into their community-based programmes. The SDM has also been included in the national family planning IEC messages and materials. Further research is required to examine the effect on other established methods of introducing the SDM, and to study the introduction of this method in a health facility service delivery setting.
In conclusion, the SDM has great potential to increase the availability and accessibility of family planning services in areas where there is low contraceptive prevalence and high unmet need for family planning. The introduction of the SDM can be undertaken effectively with the support of well-trained community-based providers. Issues that may need attention are the provision of comprehensive information and counselling for clients and potential clients.
Acknowledgments
The authors would like to acknowledge all the personnel from AGOHELD, Dilla Medan Acts, AHA and REST who demonstrated great enthusiasm and interest in collaborating in the study. The authors would also like to thank all the study participants, supervisors and data collectors who volunteered to take part in this study.
References
Footnotes
-
Funding Financial support for this study was provided by the Consortium of Reproductive Health Association (CORHA).
-
Competing interests None.
-
Ethics approval Ethics approval was obtained from the Ethical Clearance Committee of the Faculty of Medicine, Addis Ababa University (AAU). The necessary permission to undertake the study was obtained from the respective administrative regional state health bureaus (Oromiya, SNNPR and Tigray), and from the responsible bodies of Pathfinder International Ethiopia implementing partners (Dilla Medan Acts, AGOHELD, AHA and REST).
-
Provenance and peer review Not commissioned; externally peer reviewed.