Article Text

Abstract
Severe acute malnutrition (SAM) affects approximately 13 million children under the age of 5 and is associated with 1–2 million preventable child deaths each year. In most developing countries, case fatality rates (CFRs) in hospitals treating SAM remain at 20–30% and few of those requiring care actually access treatment. Recently, community-based therapeutic care (CTC) programmes treating most cases of SAM solely as outpatients have dramatically reduced CFRs and increased the numbers receiving care. CTC uses ready-to-use therapeutic foods and aims to increase access to services, promoting early presentation and compliance, thereby increasing coverage and recovery rates. Initial data indicate that this combination of centre-based and community-based care is cost effective and should be integrated into mainstream child survival programmes.
- CFR, case fatality rate
- CTC, community-based therapeutic care
- IMCI, Integrated Management of Childhood Illness strategy
- MoH, Ministry of Health
- MUAC, middle upper arm circumference
- NGO, non-governmental organisation
- NRU, nutrition rehabilitation unit
- OTP, outpatient treatment programme
- RUTF, ready-to-use therapeutic food
- SAM, severe acute malnutrition
- SC, stabilisation centre
- SFP, supplementary feeding programme
- WFH, weight-for-height
- acute malnutrition
- CTC
- SAM
Statistics from Altmetric.com
- CFR, case fatality rate
- CTC, community-based therapeutic care
- IMCI, Integrated Management of Childhood Illness strategy
- MoH, Ministry of Health
- MUAC, middle upper arm circumference
- NGO, non-governmental organisation
- NRU, nutrition rehabilitation unit
- OTP, outpatient treatment programme
- RUTF, ready-to-use therapeutic food
- SAM, severe acute malnutrition
- SC, stabilisation centre
- SFP, supplementary feeding programme
- WFH, weight-for-height
Severe acute malnutrition (SAM) is defined as a weight-for-height (WFH) measurement of <70% of the median or >3 SD below the mean National Center for Health Statistics (NCHS) reference values (termed “wasted”) or the presence of bilateral pitting oedema of nutritional origin (termed “oedematous malnutrition”).1 Many organisations also diagnose SAM when the middle upper arm circumference (MUAC) of a child between 1 and 5 years of age is <110 mm.2,3 Recently, an informal scientific committee convened by the WHO concluded that MUAC <110 mm is an independent criterion for admission to a therapeutic feeding programme for children aged 6–59 months.4 By contrast, chronic malnutrition (termed “stunted”) is identified using a height-for-age indicator and growth faltering, a composite form of malnutrition including elements of both stunting and wasting, is diagnosed using a weight-for-age indicator. These different forms of malnutrition are not only diagnosed differently but also have different causes and require different treatments. Acute malnutrition, especially SAM, is an unstable condition resulting from a relatively short duration of nutritional deficit that is often complicated by concurrent infective illness. The child with SAM has a limited ability to respond to stresses (infection and environmental), is highly vulnerable and has a high mortality risk.5,6 It is thus vital to treat SAM proactively with short duration highly intensive treatment regimes, aiming to rehabilitate the child in a few weeks. By contrast, chronic malnutrition is the result of prolonged episodes of under-nutrition both of the pregnant mother and of the young infant, most importantly during the first 2 years of life. This prolonged aetiology is best addressed through long-term preventative programmes targeting maternal health and nutrition prior to and during pregnancy, and infant health and nutrition in the first 2 years of life. These differences in aetiology, diagnosis and treatment make it important to differentiate clearly between these conditions.
THE IMPORTANCE OF ACUTE MALNUTRITION
Malnutrition in all its forms remains a major public health problem throughout the developing world and is an underlying factor in over 50% of the 10–11 million deaths in children under 5 years of age who die each year from preventable causes.7,8,9,10 Approximately 9% of sub-Saharan African and 15% of South Asian children suffer from moderate acute malnutrition11,12 and approximately 2% of children living in developing countries suffer from SAM.12 This is equivalent to roughly 60 million children suffering from moderate acute malnutrition and 13 million suffering from SAM at any one time. In India alone, approximately 2.8% of children under 5 years of age (equivalent to over 5 million children) are severely wasted,13 and in many poor countries such as Malawi, SAM is the commonest reason for paediatric hospital admission. Although data are imprecise, it is known that the risk of mortality in acute malnutrition is directly related to severity, with moderate wasting associated with a mortality rate of 30–115/1000/year6,14,15 and severe wasting associated with a mortality rate of 73–187/1000/year.14 This is equivalent to approximately 1.5 million child deaths associated with severe wasting and 3.5 million with moderate wasting every year. These figures do not include children who die of oedematous malnutrition (kwashiorkor), a form of SAM that is more common in some countries. Although these estimates are tentative, it is certain that SAM is an extremely important health problem worldwide. These data are summarised in table 1.
Worldwide burden of acute malnutrition
While the importance of under-nutrition (low weight for age) is commonly acknowledged,16 except in humanitarian relief, the importance of acute malnutrition is seldom, if ever, given sufficient importance. Vitally, SAM is not a recognised cause of death in the mortality surveillance data. As a result, none of the five papers in The Lancet child survival series that assessed the importance of illness based on these data mentioned acute malnutrition.16 This inattention extends to child survival programmes and, at present, growth monitoring programmes do not include any indicator for acute malnutrition and the Integrated Management of Childhood Illness strategy (IMCI) includes only “visible severe wasting”, an indicator that is subjective, difficult to use in practice and unreliable.17,18
The inattention paid to SAM is a serious omission. Achieving the fourth millennium development goal of a two third reduction in childhood mortality will not be possible if SAM is not addressed effectively.
THE TREATMENT OF SAM
The inpatient treatment model
For the past 30 years, the approach to treatment of SAM has focused on the clinical aspects of the condition. At present, recommended treatment regimes are exclusively inpatient, based around intensive medical and nutritional protocols administered by highly trained health care professionals in two phases (stabilisation and rehabilitation). This is the approach of the WHO management protocol1,19,20 and with minor variations forms the core of all other accepted protocols. When sufficient attention and resources, particularly skilled staff, are available, these protocols have been shown to be highly successful at rehabilitating individuals. There is good evidence that their use, combined with attention to the quality of care, can substantially decrease case fatality rates (CFRs) and their implementation in selected units in Bangladesh, South Africa and Brazil has been associated with dramatic reductions in CFRs.21–27 The same is true when they are implemented by well resourced non-governmental organisations (NGOs) during emergency humanitarian interventions.28,29 These reports underline the importance of appropriate protocols, in particular the provision of gram negative cover for cases of SAM with complications, in effective management. However, they also indicate that even in these relatively affluent countries, the availability of skilled, motivated and well trained staff and other resources are vital determinants of successful implementation.
Despite the success of these protocols when implemented in selected units, their publication has not led to a widespread decrease in CFRs in most hospitals in the developing world.30,31 To date, CFRs in the vast majority of health facilities in developmental settings remain at 20–30% for marasmus and up to 50–60% for kwashiorkor,32 slightly higher than those seen in the 1950s.33 The persistence of such high CFRs is generally attributed to inappropriate case management as a result of poor knowledge34 and the accepted view is that wider implementation of the WHO guidelines through in-service training and incorporation into medical and nursing curricula is the key towards decreasing CFRs worldwide.13,35–37
However, in most countries where SAM is common there are insufficient skilled and motivated staff available to implement these protocols on the scale that is required. Table 2 presents the numbers of nurses and doctors in some of the African countries most affected by SAM, comparing them to South African staffing standards. This table indicates that in 20 of the African countries most affected by acute malnutrition, there are on average less than 22 nurses and 4 doctors/100 000 population, <10% of the staff available in South Africa.38
Physicians and nurses, density per 100 000 population and a comparison of this density with that in South Africa
The low numbers of trained health staff have been identified as a fundamental constraint to improving health outcomes and reaching the millennium development goals.39 In practice, insufficient numbers of skilled health staff usually preclude the effective and sustainable implementation of the WHO guidelines for the treatment of SAM.
Such problems with the exclusive inpatient treatment of SAM are not new. Since the 1960s, the high cost and poor success rates of hospital inpatient treatment have prompted continued debate over whether hospitals are the best place to treat such patients.40–42 Limited inpatient capacity, and low numbers of trained staff available in hospitals to treat the large numbers requiring care, has long been known to limit impact and programme coverage.43,44 The centralised nature of hospitals also promotes late presentation, high opportunity costs for carers and serious risks of cross infection for immunosuppressed children with SAM congregated in wards. The result has been high mortality rates and low coverage of services.33,45–47 These problems are still essentially the same today.48
Community-based therapeutic care
During the past 5 years, an increasing number of countries and international relief agencies have adopted a community-based model for the management of acute malnutrition, called community-based therapeutic care (CTC).49,50 The CTC model consists of four elements:
-
Measures to mobilise the community in order to encourage early presentation and compliance;
-
Outpatient supplementary feeding protocols for those with moderate acute malnutrition and no serious medical complications;
-
Outpatient therapeutic protocols for those with severe acute malnutrition and no serious medical complications; and
-
Inpatient therapeutic protocols for those with acute malnutrition also suffering from serious medical complications.
Together with the criteria determining patient flow between these elements, the CTC model of care provides a framework for an integrated public health response to acute malnutrition. Experience over the past 5 years indicates that when sufficient attention is given to early case finding, most cases of SAM can be successfully treated solely as outpatients, enabling resource intensive inpatient care to be reserved for the minority suffering from SAM with complications.48 This allows for scarce resources to be used more cost effectively. The CTC model also aims to integrate treatment with a variety of other interventions designed to reduce the incidence of malnutrition and improve public health and food security. CTC programme design attempts to take into account the socio-economic factors, particularly poverty, high workloads for women and the relative exclusion from health and education services that contribute to the late presentation of cases of acute malnutrition. Programmes are therefore highly decentralised in order to minimise geographical barriers to access48 and include intensive community consultation and mobilisation to maximise understanding and participation. This design minimises the costs to families and maximises access to treatment.51 The decentralised design also means that, in non-emergency situations, there are few cases of SAM at any one access point. This means that the quantities of ready-to-use therapeutic food (RUTF) required to treat patients are therefore small and can be easily delivered together with other routine health supplies. This facilitates the integration of CTC into existing health services. In current Ministry of Health (MoH) implemented programmes in Malawi, for example, a health centre treating 15 children per month requires 160 kg (eight boxes) of RUTF, easily deliverable by routine MoH logistics.
Results of CTC
Emergency programmes
CFRs among 23 511 unselected severely malnourished children treated in 21 CTC programmes operating in Malawi, Ethiopia and Sudan, between 2001 and 2005, were 4.1%, with recovery rates of 79.4% and default rates of 11.0%. Transfer and non-recovery rates were 3.3% and 2.2%, respectively. Some 76% of these severely malnourished children were treated solely as outpatients.4,49,50 These results are presented in table 3. Coverage rates for nine of these programmes have been estimated using the centric systematic area sampling (CSAS) method, a new direct method for assessing coverage.52 Average coverage was 72.5%,4,50 substantially higher than coverage rates seen in comparable centre-based programmes which are often less than 10%.53,54 Similar positive results have recently been published from Niger, where Médecins sans Frontières (MSF) cared for more than 60 000 children with SAM using an approach based on an outpatient treatment programme (OTP) design. Approximately 70% of these children were treated solely as outpatients and overall CFRs were approximately 5%.55
CTC outcomes of severely malnourished children aged under 59 months presenting to CTC programmes between September 2000 and December 2005 (n = 23 511)
CTC results in non-emergency programmes
Achieving long-term improvements in the treatment of SAM on a large scale requires that community-based management of SAM is implemented from existing MoH structures as a standard part of the primary health care package. The first two large CTC programmes implemented in stable situations, in Dowa district in Malawi and in South Wollo in Ethiopia, have now been operating for 4 years. From the outset, OTP services were delivered through the local MoH clinics, and local hospitals provided stabilisation care for children suffering from SAM with complications. Initially NGO teams from Concern Worldwide heavily supported this implementation, but after the emergency phase this support has been progressively reduced. In Wollo, as of mid 2005, the only external inputs were the purchase and transport of RUTF, intermittent monitoring/research inputs and support for eight of the original 35 outreach workers. The MoH has been responsible for the implementation of OTP services through their clinics and has continued to run the inpatient stabilisation centre operating in the district hospital. The outcomes up to May 2005 are presented in table 4 and indicate that recovery rates have remained high during this transition period and still exceed international standards. In January 2005, 9 months into this transition, programme coverage rates for severely malnourished children were 77.3% (95% CI 72.0% to 82.2%),56 similar to those of 77.5% (95% CI 65.7% to 86.2%) obtained in June 2004 at a time when Concern Worldwide was heavily involved.57
Outcomes from the clinical cards of severely malnourished children presenting to the CTC programme in Wollo Ethiopia, February 2003–May 2005 (n = 2498*)
Similar results have been obtained in Malawi where, 2 years into the handover from NGO to MoH control, programme outcomes still exceed international standards for therapeutic feeding programmes with a 75.7% recovery rate and 5.9% mortality rate overall. Coverage rates have also remained high and in June 2004 were 72.2% (95% CI 66.4% to 78.0%),58 similar to the results of 73.64% (95% CI 66.0% to 81.3%) obtained in March 2003 at the height of NGO support.59 These and similar experiences with CTC have resulted in both the Malawi and Ethiopian governments developing national guidelines based on CTC.
Several factors have facilitated integration into primary health care. The simplicity of the OTP protocols, the ease with which they can be taught to local clinic staff and the ease with which they can be implemented are all critical determinants of success. Protocols must be kept as simple and as fast as possible to implement if busy clinic staff are to adopt them. Integrating CTC into annual “district implementation plans” with sufficient budgets for the logistics of RUTF transport, supervision, refresher training and monitoring is also important. Building understanding and participation among local people improves passive case finding and promotes more appropriate and earlier presentation at clinics. This decreases staff time spent on screening and improves the clinical effectiveness of the OTP protocols, in turn improving results and leading to better staff retention. Decentralisation and fostering easier access and earlier presentation also reduces the numbers of cases presenting with complications and has had similar positive effects on outcomes and morale. Facilitation of community-based screening and the use of MUAC measurement for both screening and admission have decreased the number of people who are wrongly referred from village level screening. This reduces the negative feedback from those who have wasted their time and efforts attending a clinic after being inappropriately referred. This has improved programme acceptability and the appropriate presentation and uptake of services.
These initial results are encouraging. It is important to note, however, that CTC is a new mode and further data collection and analysis of the factors that facilitate integration of CTC into primary health care delivery are required.
The cost of CTC
Programmes treating SAM precisely target resources at children with a very high mortality risk and therefore tend to be highly cost effective in terms of additional years of life gained. Initial data indicate that the cost-effectiveness of emergency CTC programmes is comparable to mainstream child survival interventions such as vitamin A provision or oral rehydration therapy for diarrhoeal disease. Initial estimates from two established emergency CTC programmes varied between US$12 and US$132 for each year of life gained, equivalent to US$101–US$197 per admission.60 The exact figure depended on the density and prevalence of SAM, the numbers of acutely malnourished patients treated, the infrastructure present, accessibility and the estimation of CFR in untreated SAM used in the calculation.4,60 Although these are broad ranges, the highest cost is below the US$150 threshold described by the World Bank as highly cost effective. The development of local production of RUTF, using new recipes based upon locally available grains and pulses, should further reduce costs. Other cost data comparing the community-based treatment of severe malnutrition with centre-based care come from Bangladesh in the 1990s. In this study, the cost of community-based rehabilitation was approximately 25% of the cost of inpatient care.61 However, this programme did not provide any nutritional supplements for those treated in the community. The additional cost of 10–15 kg of RUTF (the average amount required to obtain a cure in OTP), of approximately US$35–US$52.5 would still have resulted in a 50% reduction in inpatient costs.
THE DETERMINANTS OF SUCCESSFUL TREATMENT
Early presentation
The severity of SAM, its prognosis and the determinants of successful treatment are primarily dependent on the lead time to presentation.6,15,44,62–64 If malnourished people access nutritional care early in the evolution of their condition and comply with treatment until they have recovered, success rates are high. Conversely, if people access care late and/or they are deterred from staying in the programme for as long as necessary, then success rates are low. In practice, this means that the actual clinical protocols used are not the most crucial determinants of success. Instead, designing programmes so that cases present early on during the progression of their condition is the major factor behind successful treatment. This has important practical consequences for resource requirements and effectiveness. As the clinical evolution of acute malnutrition progresses, treatment must become increasingly intensive (and costly) if it is to succeed. Centralised inpatient units treating SAM are frequently confronted by extremely ill patients who require intensive medical and nursing care. Most of these are in the poorest parts of the poorest countries in the world and have severe resource and staff constraints. In addition, the carers of the malnourished patients almost always come from the poorest families. These people have great demands on their time and cannot afford to leave home for long periods to stay with their malnourished child during prolonged inpatient treatment.
If on the other hand, cases of SAM are caught in the early stages of their evolution, at a stage when the child still has a good appetite, the technical aspects of treatment are simple. All that is required is a balanced diet of sufficient quantity and quality in terms of protein, carbohydrate, fat and micronutrients. The composition of such diets is now well developed and for the past 10 years the WHO has recommended a milk-based diet called F100 for the “recovery phase” of treatment.
Energy- and nutrient-dense rehabilitation diets
The provision of energy- and nutrient-dense foods, including sufficient micronutrients, is a vital determinant of the successful treatment of SAM. F100, although extremely effective at rehabilitating individual cases of SAM in inpatient centres, is very vulnerable to bacterial contamination and, as a result, must be used within a couple of hours of being made up. This restricts its use to inpatient facilities. The development in the mid 1990s of RUTF65 has greatly eased the difficulties associated with providing a suitable high energy, nutrient-dense food that is safe to use in outpatient programmes. RUTF is an energy-dense, mineral and vitamin-enriched food, with a similar nutrient profile but greater energy and nutrient density than F100.65 In contrast to the water-based F100, RUTF is an oil-based paste with extremely low water activity.66 As a result, bacteria do not grow in RUTF even when accidentally contaminated,67 allowing it to be kept un-refrigerated in simple packaging for several months. As RUTF is eaten uncooked, heat labile vitamins are not destroyed during preparation and the labour, fuel and water demands on poor households are minimised. The production process is simple and RUTF can be made from local crops68 using basic technology that is readily available in developing countries.69,70
In a clinical trial of severely malnourished children undertaken in Senegal, energy intakes (808 vs 573 kJ/kg/day, p<0.001), rates of weight gain (15.6 vs 10.1 g/kg/day, p<0.001) and time to recovery (17.3 vs 13.4 days, p<0.001) were all significantly greater in those receiving RUTF than in those receiving F100.71 Trials in Malawi have also successfully used RUTF as a take-home ration given to children in the recovery phase of the treatment of SAM. In one trial, an RUTF take-home ration of 730 kJ/kg/day (175 kcal/kg/day) successfully rehabilitated HIV negative severely malnourished children, after early discharge from a nutrition rehabilitation unit (NRU) providing phase one care according to WHO protocols. Rates of weight gain (5.2 vs 3.1 g/kg/day) and the proportion of children recovering to 100% WFH were significantly higher in the RUTF groups when compared to groups receiving a larger amount of energy from corn/soya blend flour supplied by the World Food Programme (95% vs 78%, RR 1.2, 95% CI 1.1 to 1.3).72 In the same trial, 56% of the HIV positive children treated with RUTF also achieved 100% WFH.73 In another trial implemented in rural NRUs, 730 kJ/kg/day (175 kcal/kg/day) of locally made RUTF given during the rehabilitation phase of treatment, produced significantly better rates of weight gain (3.5 vs 2.0 g/kg/day), recovery (79% vs 46%, RR 2.8, 95% CI 2.5 to 3.1) and mortality (3.0 vs 5.4%, OR 0.5, 95% CI 0.3 to 0.7) than the standard inpatient treatment using F100, followed by outpatient supplementation with a large one-off ration (50 kg) of corn/soya blend flour.74 The rates of weight gain on the RUTF regime were far lower than the 10–15 g/kg/day that should be achieved under optimal conditions with a ration of 730 kJ/kg/day. The combination of low rates of weight gain and low mortality rates indicates that this was probably due to sharing of the RUTF ration.
By shortening the duration of inpatient treatment from an average of 30 days to only 5–10 days, the recent move towards using RUTF in the recovery phase of treatment reduces the resources, both staff and materials, needed to treat SAM. This improves cost-effectiveness. The provision of phase one inpatient care for all cases, however, still requires substantial resources and entails relatively large opportunity costs for carers. A requirement for inpatient care also means that programmes must be implemented from hospitals and large clinics with inpatient facilities. This centralises treatment, increasing barriers to access for the majority of rural communities where acute malnutrition is usually most prevalent. Increased barriers to access and opportunity costs serve to delay presentation, making the condition harder to treat and increasing the proportion of patients with complications. This increases programme costs and CFRs.64 These barriers also decrease the proportion of severely malnourished children who are able to access treatment, thereby reducing programme coverage.
Matching intensity of care to clinical needs
In order for resources to be targeted in the most cost effective manner, it is essential to differentiate between those who need inpatient care and those who will survive when given appropriate assistance on an outpatient basis. In the CTC approach, SAM is sub-divided based on whether there are co-existent life threatening complications75 (fig 1). Children presenting with SAM complicated by life threatening illness are admitted into “stabilisation centres” where they receive inpatient care based on the WHO inpatient treatment protocols. Those with SAM but without life threatening complications (usually 80–90% of presentations) are treated solely as outpatients through weekly or fortnightly attendance in OTPs. In the OTP, they receive a 200 kcal/kg/day take-home ration of RUTF, a course of oral broad-spectrum antibiotics, vitamin A, folic acid, anti-helminthics and if appropriate, anti-malarials. This division of SAM is important to optimise the effectiveness of treatment. Treating patients with SAM without complications solely as outpatients greatly reduces the demand for skilled staff and resources. It also reduces the costs to families and carers associated with accessing treatment, thereby encouraging early presentation and promoting successful treatment.
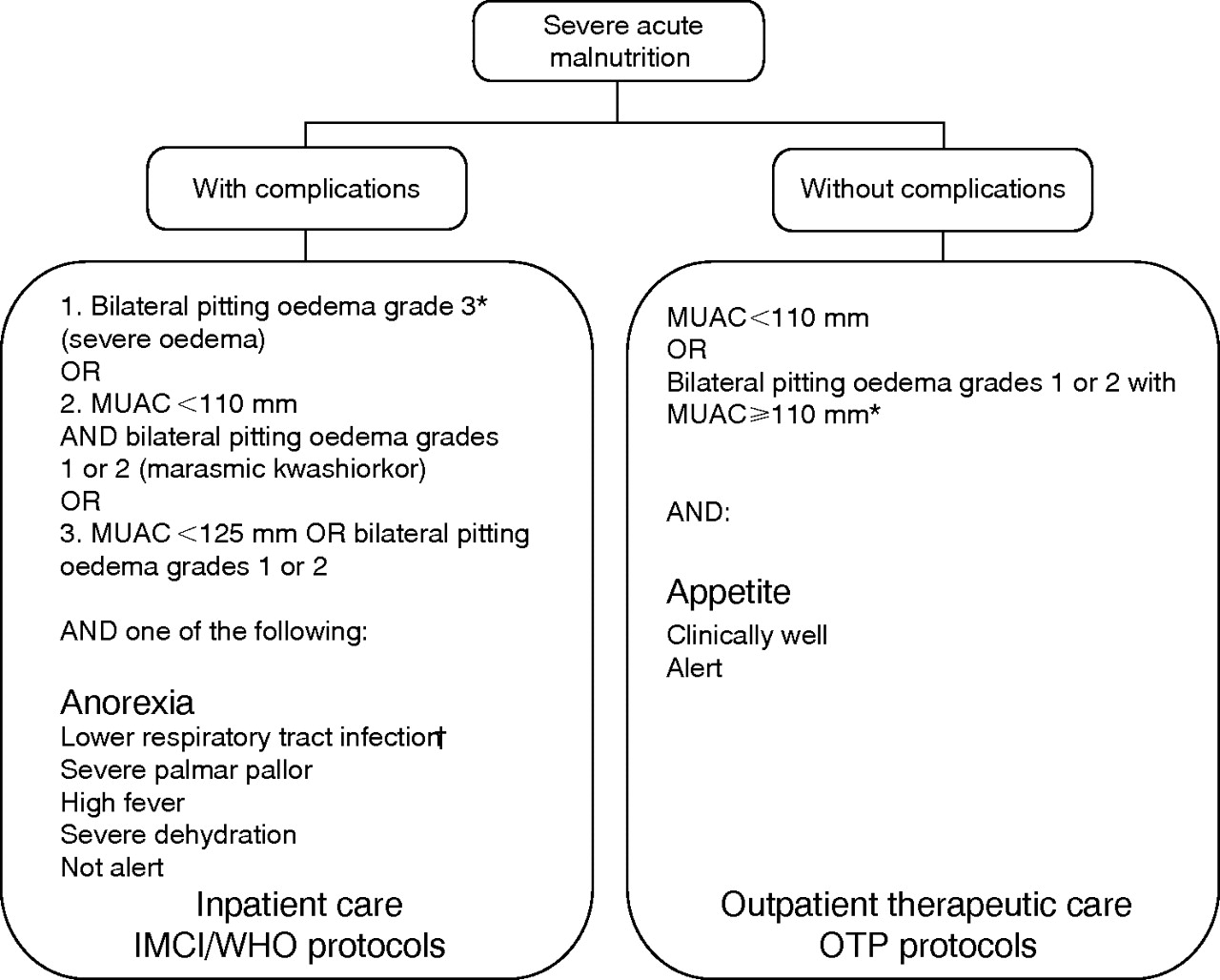
{kind=link}
Classification of severe acute malnutrition used in CTC programmes. *Grade 1 oedema is mild oedema on both feet/ankles; grade 2 is moderate oedema on both feet, plus lower legs, hands or lower arms; and grade 3 is severe generalised oedema including both feet, legs, hands, arms and face. †For children between children 6–59 months or 65–110 cm as a proxy of age.
Access, understanding and participation
In order to present early and comply with treatment, people must be able to access care. People must have physical access to the service, they must understand what the service does and be aware of the implications that their use of the service will have on their day-to-day lives. Physical barriers to access and compliance can be overcome by providing care close to where the target population lives. In the developmental setting, this involves delivering the service through the front line primary health care structures such as local clinics, health posts or temporary expanded programme on immunisation (EPI) vaccination points. In humanitarian responses it often involves creating new temporary OTP access points. Promoting understanding among the target population requires that service providers themselves invest in understanding the socio-cultural milieu in which they operate. Then they must engage with the local population to communicate clearly, using appropriate channels and methods of communication, what the service does and what it entails. The investments required are not necessarily expensive or particularly time consuming, but they have to be planned properly and have sufficient appropriate resources allocated to them.
Experiences during the development of CTC have indicated that upfront investment in social mobilisation is needed if programmes are to successfully move towards sustainability. The aim is to ensure that key stakeholders participate in the programmes so that they can directly benefit from the positive feedback and kudos associated with curing sick children. This positive feedback is vital if programmes are to generate sufficient and self-perpetuating motivation to sustain early presentation and compliance. The nature of SAM offers unrivalled potential for this to happen and there is no other condition that is potentially so devastating to families but so easily treated with simple understandable measures (quality therapeutic food) delivered by the families themselves. This unparalleled potential to motivate health staff and community members is a key advantage that CTC has over other community-based interventions. This potential must be cultivated right from the start of programmes and requires appropriate resources and engagement with the communities, key stakeholders and local health care providers. This is necessary to build understanding, trust and participation among all groups to ensure that programmes are designed to reflect the priorities, constraints and resources of the target population. The use of MUAC as the sole anthropometric indicator for screening and admission into CTC programmes facilitates this, helping to devolve responsibility for patient selection towards the community. MUAC is an indicator of acute malnutrition that reflects mortality risk18,63,76 and has recently been endorsed as an independent criterion for admission into therapeutic feeding programmes by an informal consultation of the WHO.4,18 The use of MUAC does not require the use of complicated equipment and can easily be taught to un-educated community-based workers making it practical for use in resource-poor settings.77,78
CONCLUSION
Where sufficient resources are made available, the WHO inpatient medicalised treatment model for SAM can achieve low CFRs. However, exclusive inpatient treatment strategies are resource intensive, requiring large numbers of skilled staff. As the prevalence of SAM is highest in resource-poor environments, there is usually a substantial mismatch between the large numbers of patients requiring treatment and the small numbers of skilled staff and limited resources available to treat them. The HIV/AIDS pandemic is further reducing resource availability and increasing the numbers of acutely malnourished patients, aggravating this mismatch and increasing CFRs.
CTC complements the existing WHO inpatient protocols, using RUTFs to treat most children suffering from SAM solely as outpatients and reserving inpatient treatment for those with complications. RUTF is relatively cheap to produce and so long as the patient has an appetite, easy to administer, making success rates high and costs per treatment low. CTC is designed to decrease barriers to access, encourage earlier presentation, reduce opportunity costs associated with treatment and encourage patient compliance. Treating most cases of SAM solely as outpatients reduces inpatient caseloads to more manageable levels. This helps decongest crowded inpatient units, decreases the risks of nosocomial infection and increases the time available to staff to devote to the sickest children. This new approach has dramatically reduced CFRs and increased coverage rates. Initial data indicate that it has improved the cost-effectiveness of treating SAM.
CTC should now be scaled up in both emergency and non-emergency settings and appropriate training included in medical, nursing and primary health care curricula. The WHO, UNICEF and the UN Standing Committee on Nutrition recently convened an informal consultation on the community-based management of severe malnutrition in children. The meeting began the process of incorporating the techniques into the WHO guidelines.4 This is an essential step. However, improvements in treatment protocols, programme design and training by themselves are insufficient. If CTC is to attain its maximum potential in reducing avoidable child mortality, there must be changes in funding priorities and child survival strategies. Leveraging these changes will require strong evidenced-based advocacy, highlighting the global importance of SAM and communicating clearly the fact that highly cost-effective interventions exist.
To facilitate this, the WHO should adopt the term “acute malnutrition” in order to differentiate wasting and oedematous malnutrition from severe growth faltering and stunting. This is important, as acute malnutrition has different causes, different indicators and requires different interventions to those for chronic malnutrition. Without a clear and appropriate nomenclature these differences are obscured, resulting in confusion over treatment strategies and mixed messages going out to policy makers.
Secondly, the global importance of SAM as a major cause of avoidable mortality must be better communicated and the child survival agenda must give greater priority to treating the condition. This requires SAM to be included as a specific cause of death in mortality surveillance data. Without this, the high numbers of deaths attributable to SAM will continue to go unrecorded and unnoticed.
Thirdly, nutritionists should communicate the fact that high impact, highly cost-effective interventions exist to treat SAM. Although the hospital-based treatment of SAM has long been shown to be cost effective, and cheaper than many of the mainstream child survival interventions such as treatment of severe diarrhoea in hospitals or vitamin A distribution,54,79 this has been poorly communicated to policy makers and funders. CTC promises to increase this cost-effectiveness further and there is a need for more cost-effectiveness data to better document this.
Lastly, an appropriate indicator of acute malnutrition such as MUAC should be included as a standard element in both growth monitoring programmes and IMCI, in order to allow these programmes to diagnose acute malnutrition more effectively. This is essential if cases of SAM are to be caught early, before complications arise and while cheap outpatient treatment is possible. At present, growth monitoring programmes do not include any indicator of acute malnutrition and IMCI includes only “visible severe wasting”, an indicator that is subjective, difficult to use in practice and unreliable.17,18 MUAC is easy to use and efficient at identifying those children who require specialist interventions. Without this, the majority of cases of SAM will continue to go undiagnosed and untreated.
Achieving the fourth millennium development goal of a two third reduction in childhood mortality will not be possible if SAM is not addressed effectively. Cost-effective, high impact approaches now exist. In order for these to reach their potential, the treatment of SAM must become more central to the health care agendas in developing countries. Policy makers, health care funders and health professionals must accord SAM an importance and urgency commensurate with its global significance as a leading cause of preventable childhood mortality and morbidity.
REFERENCES
Footnotes
-
Funding: This work was supported by funding from Concern Worldwide. Concern Worldwide has been engaged in the research and development of community-based therapeutic care but has had no influence over the text of this review.
-
Competing interests: The author works for Valid International Ltd, an organisation that has been engaged in the research and development of community-based therapeutic care. He is also an unpaid director of Valid Nutrition, a not-for-profit company established to research and manufacture ready-to-use therapeutic food in developing countries.