
Screening People with Tuberculosis for High Risk of Severe Illness at Notification: Programmatic Experience from Karnataka, India

 , , and
, , and
Abstract
:1. Introduction
- 1.
- BMI < 14.0 kg/m2
- 2.
- MUAC < 16.0 cm (if unable to stand for a measurement of weight and height)
- 3.
- BMI 14.0–15.9 kg/m2 AND (bilateral pedal oedema OR inability to stand without support OR no appetite)
- 4.
- MUAC 16.0–18.9 cm AND (bilateral pedal oedema OR inability to stand without support OR no appetite)
- 5.
- Severe anaemia (Hb < 7 g/dL) with or without heart failure
- 6.
- Unstable vital signs–pulse rate > 100 per minute OR RR > 24 per minute OR oxygen saturation < 94% OR systolic blood pressure < 100 mm Hg OR poor performance status (bed-ridden or extremely limited mobility)
- 7.
- Complications of PTB–Example, moderate–massive haemoptysis, hydro-pneumothorax
- 8.
- Complications of EPTB–Example, altered consciousness, seizures, lower limb weakness, suspected intestinal obstruction or perforation
- 9.
- Complications to anti-TB treatment–drug induced hepatotoxicity or seizures
- 10.
- Patients with comorbidities who need inpatient care to manage these comorbidities according to the judgement of the treating physician–Example, DM, HIV, liver or renal disease, alcohol addiction, tobacco addiction
- TB—tuberculosis, BMI—body mass index (kg/m2), MUAC—mid upper arm circumference (cm), Hb—haemoglobin, RR—respiratory rate, PTB—pulmonary TB, EPTB—extra pulmonary TB, DM—diabetes mellitus, HIV—human immunodeficiency virus.
- 1.
- Body mass index (BMI) less than or equal to (≥) 14.0 kg/m2# (OR)
- 2.
- BMI less than or equal to (≥) 16.0 kg/m2 with leg swelling# (OR)
- 3.
- Respiratory rate more than (>) 24 per minute## (OR)
- 4.
- Oxygen saturation less than (<) 94% ## (OR)
- 5.
- Not able to stand without support (standing with support/squatting/sitting/bed ridden)
- TB—tuberculosis; # very severe undernutrition indicators; ## respirator insufficiency indicators.
2. Materials and Methods
2.1. Study Design and Participants
2.2. Setting
2.3. Screening Tool
2.4. Data Collection, Variables and Sources of Data
2.5. Data Management
2.6. Statistics
3. Results
3.1. Baseline Characteristics of Notified Patients
3.2. Feasibility Indicators for Screening of Severe Illness in Routine Settings
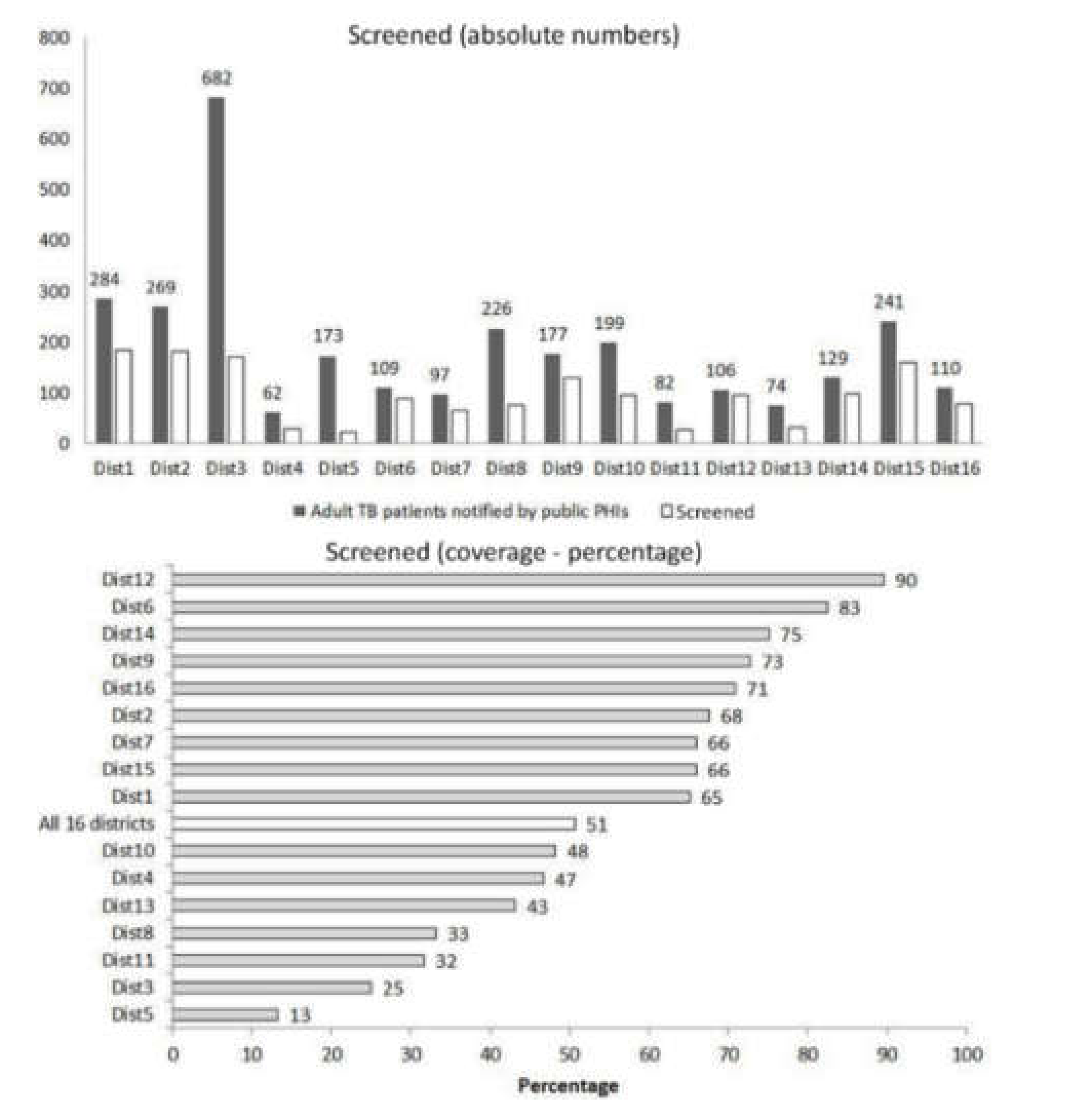
3.2.1. Coverage of Screening and Factors Associated
3.2.2. Delays in Screening
3.2.3. Errors in Data Collected and Missing Data
3.3. Burden of ‘High Risk of Severe Illness’
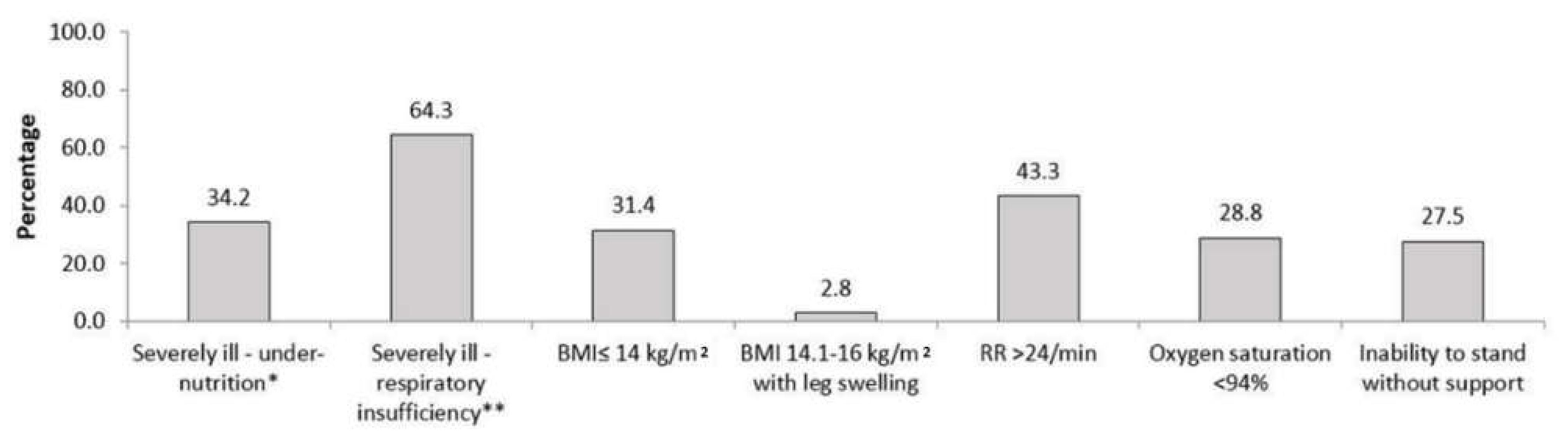
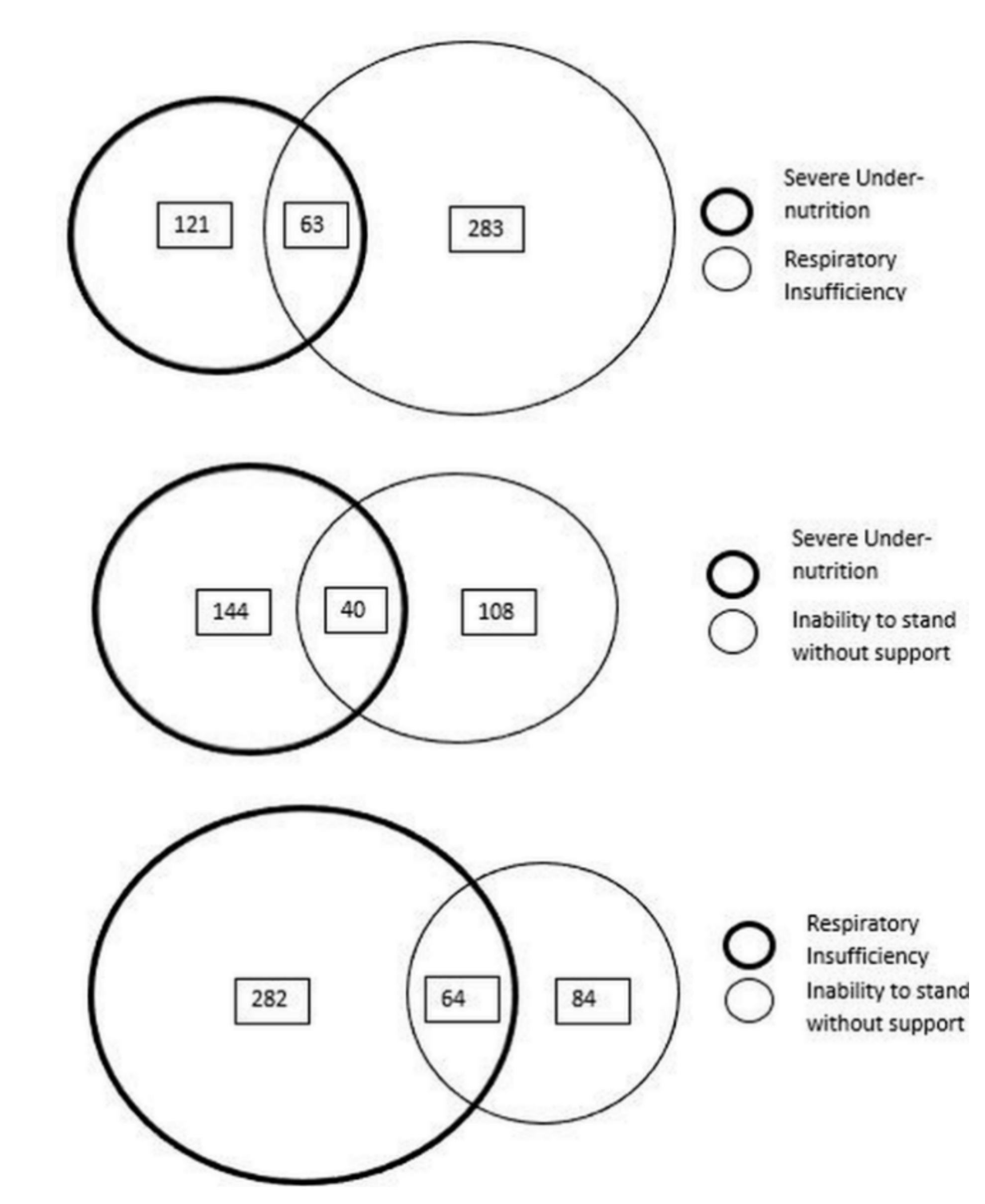
3.4. Contribution of Various Indicators to ‘High Risk of Severe Illness’
4. Discussion
4.1. Strengths and Limitations
4.2. Key Findings
4.3. Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- World Health Organization (WHO). Global Tuberculosis Report 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization (WHO). End TB Strategy: Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Word Health Organization (WHO). Health in 2015 from Millennium Development Goals (MDG) to Sustainable Development Goals (SDG); WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Cullinan, P.; Meredith, S.K. Deaths in adults with notified pulmonary tuberculosis 1983-5. Thorax 1991, 46, 347–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shuldiner, J.; Leventhal, A.; Chemtob, D.; Mor, Z. Mortality of tuberculosis patients during treatment in Israel, 2000–2010. Int. J. Tuberc. Lung Dis. 2014, 18, 818–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, N.; Lim, M.S.C.; Murray, J.; Dowdeswell, R.J.; Glynn, J.R.; Sonnenberg, P. Timing, rates, and causes of death in a large South African tuberculosis programme. BMC Infect. Dis. 2014, 14, 3858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Nam, H.W.; Choi, S.H.; Yoo, S.S.; Lee, S.Y.; Cha, S.I.; Park, J.Y.; Kim, C.H. Comparison of Early and Late Tuberculosis Deaths in Korea. J. Korean Med. Sci. 2017, 32, 700–703. [Google Scholar] [CrossRef] [PubMed]
- Adamu, A.L.; Gadanya, M.A.; Abubakar, I.S.; Jibo, A.M.; Bello, M.M.; Gajida, A.U.; Babashani, M.M.; Abubakar, I. High mortality among tuberculosis patients on treatment in Nigeria: A retrospective cohort study. BMC Infect. Dis. 2017, 17, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, J.; Kim, J.S.; Kim, H.W.; Shin, A.Y.; Koo, H.-K.; Lee, S.-S.; Kim, Y.-K.; Shin, K.-C.; Chang, J.H.; Chun, G.; et al. Clinical profiles of early and tuberculosis-related mortality in South Korea between 2015 and 2017: A cross-sectional study. BMC Infect. Dis. 2019, 19, 735. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira, S.P.; Da Silveira, J.T.P.; Beraldi-Magalhães, F.; De Oliveira, R.R.; De Andrade, L.; Cardoso, R.F. Early death by tuberculosis as the underlying cause in a state of Southern Brazil: Profile, comorbidities and associated vulnerabilities. Int. J. Infect. Dis. 2019, 80, S50–S57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Global Tuberculosis Report 2019; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Bhargava, A.; Bhargava, M. Tuberculosis deaths are predictable and preventable: Comprehensive assessment and clinical care is the key. J. Clin. Tuberc. Other Mycobact. Dis. 2020, 19, 100155. [Google Scholar] [CrossRef] [PubMed]
- Bhargava, M.; Bhargava, A.; Akshaya, K.M.; Shastri, S.G.; Bairy, R.; Parmar, M.; Sharath, B.N. Nutritional assessment and counselling of tuberculosis patients at primary care in India: Do we measure up? Int. J. Tuberc. Lung Dis. 2019, 23, 147–150. [Google Scholar] [CrossRef]
- Central TB Division. Guidance Document on Nutritional Care and Support for Patients with Tuberculosis in India; Ministry of Health and Family Welfare: New Delhi, India, 2017.
- Central TB Division. Technical Guidance for Comprehensive Package for Differentiated Care for TB Patients; Ministry of Health and Family Welfare: New Delhi, India, 2021.
- Valade, S.; Raskine, L.; Aout, M.; Malissin, I.; Brun, P.; Deye, N.; Baud, F.J.; Megarbane, B. Tuberculosis in the intensive care unit: A retrospective descriptive cohort study with determination of a predictive fatality score. Can. J. Infect. Dis. Med. Microbiol. 2012, 23, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, H.N.; Osório, N.S.; Castro, A.G.; Ramos, A.; Carvalho, T.; Meira, L.; Araújo, D.; Almeida, L.; Boaventura, R.; Fragata, P.; et al. A Prediction Rule to Stratify Mortality Risk of Patients with Pulmonary Tuberculosis. PLoS ONE 2016, 11, e0162797. [Google Scholar] [CrossRef] [Green Version]
- Central TB Division. National Strategic Plan for TB Elimination 2017-25; Ministry of Health and Family Welfare: New Delhi, India, 2017. [Google Scholar]
- Bhargava, A.; Shewade, H.D. The societal impact of the COVID-19 response related lockdown on TB incidence and mortality in India. Indian J. Tuberc. 2020. in review. [Google Scholar] [CrossRef] [PubMed]
- Institute of Population Sciences and Ministry of Health and Family Welfare (Government of India). Fact Sheet: Key Indicators, 22 States/UTs from Phase I. National Family Health Survey 2019-20 (NFHS 5); Ministry of Health and Family Welfare: New Delhi, India, 2020.
- Central TB Division. India TB Report 2020: National Tuberculosis Elimination Programme; Annual Report; Ministry of Health and Family Welfare: New Delhi, India, 2020.
- National TB Elimination Programme; India Nikshay Reports. Available online: https://reports.nikshay.in/Reports/TBNotification (accessed on 2 January 2020).
- De Vallière, S.; Barker, R.D. Poor performance status is associated with early death in patients with pulmonary tuberculosis. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Horita, N.; Miyazawa, N.; Yoshiyama, T.; Kojima, R.; Omori, N.; Kaneko, T.; Ishigatsubo, Y. Poor performance status is a strong predictor for death in patients with smear-positive pulmonary TB admitted to two Japanese hospitals. Trans. R. Soc. Trop. Med. Hyg. 2013, 107, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Waitt, C.J.; Squire, S.B. A systematic review of risk factors for death in adults during and after tuberculosis treatment. Int. J. Tuberc. Lung Dis. Off. J. Int. Union Tuberc. Lung Dis. 2011, 15, 871–885. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Management of Severe Malnutrition: A Manual for Physicians and Other Senior Health Workers; WHO: Geneva, Switzerland, 1999.
- Shastri, S.; Naik, B.; Shet, A.; Rewari, B.; De Costa, A. TB treatment outcomes among TB-HIV co-infections in Karnataka, India: How do these compare with non-HIV tuberculosis outcomes in the province? BMC Public Health 2013, 13, 838. [Google Scholar] [CrossRef] [Green Version]
- Bhargava, A.; Chatterjee, M.; Jain, Y.; Chatterjee, B.; Kataria, A.; Bhargava, M.; Kataria, R.; D’Souza, R.; Jain, R.; Benedetti, A.; et al. Nutritional status of adult patients with pulmonary tuberculosis in rural central India and its association with mortality. PLoS ONE 2013, 8, e77979. [Google Scholar] [CrossRef] [PubMed]
- Nirgude, A.S.; Kumar, A.M.V.; Collins, T.; Naik, P.R.; Parmar, M.; Tao, L.; Akshaya, K.M.; Raghuveer, P.; Yatnatti, S.K.; Nagendra, N.; et al. “I am on treatment since 5 months but I have not received any money”: Coverage, delays and implementation challenges of “Direct Benefit Transfer” for tuberculosis patients—A mixed-methods study from South India. Glob. Health Action 2019, 12, 1633725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, B.H.; Jeyashree, K.; Chinnakali, P.; Vijayageetha, M.; Mehta, K.G.; Modi, B.; Chavda, P.D.; Dave, P.V.; Zala, C.C.; Shewade, H.D.; et al. Cash transfer scheme for people with tuberculosis treated by the National TB Programme in Western India: A mixed methods study. BMJ Open 2019, 9, e033158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhargava, A.; Bhargava, M.; Pande, T.; Rao, R.; Parmar, M. N-TB: A mobile-based application to simplify nutritional assessment, counseling and care of patients with tuberculosis in India. Indian J. Tuberc. 2019, 66, 193–196. [Google Scholar] [CrossRef] [PubMed]
- Press Information Bureau. Government of India Cabinet Approves Ayushman Bharat—National Health Protection Mission. Available online: http://pib.nic.in/newsite/PrintRelease.aspx?relid=177816 (accessed on 31 March 2018).




{kind=link}
{kind=link}
{kind=link}
| Characteristics * | n | (%) | |
|---|---|---|---|
| Total | 3020 | (100.0) | |
| Demographic characteristics | |||
| Age in years | |||
| 15–24 | 476 | (15.8) | |
| 25–34 | 611 | (20.2) | |
| 35–44 | 619 | (20.5) | |
| 45–54 | 575 | (19.0) | |
| 55–64 | 416 | (13.8) | |
| ≥65 | 323 | (10.7) | |
| Gender | |||
| Men | 2039 | (67.5) | |
| Women | 981 | (32.5) | |
| Clinical characteristics | |||
| Test used for diagnosis | |||
| Xpert MTB/RIF | 1423 | (47.1) | |
| TrueNat MTB/RIF | 190 | (6.3) | |
| LPA | 17 | (0.6) | |
| Microscopy | 557 | (18.4) | |
| Culture | 9 | (0.3) | |
| Chest Radiograph | 272 | (9.0) | |
| Others | 552 | (19.3) | |
| Bacteriological confirmation (yes) | 2284 | (75.6) | |
| Site | |||
| Pulmonary | 2186 | (72.4) | |
| Extrapulmonary | 667 | (22.1) | |
| Missing | 167 | (5.5) | |
| Previous treatment (yes) | 474 | (15.7) | |
| HIV | |||
| Positive | 225 | (7.5) | |
| Negative | 2531 | (83.8) | |
| Unknown | 264 | (8.7) | |
| DM | |||
| Yes | 505 | (16.7) | |
| No | 2086 | (69.1) | |
| Unknown | 429 | (14.2) | |
| Health system characteristics | |||
| Bank details available with programme (yes) | 2353 | (77.9) | |
| Peripheral Health Institute–notification facility | |||
| District/Teaching hospital | 1942 | (66.6) | |
| Sub-district level hospital | 769 | (26.4) | |
| Primary health centre | 206 | (7.1) | |
| Days to notify from diagnosis | |||
| Within a day | 2160 | (71.5) | |
| 1–6 days | 632 | (20.9) | |
| 7–13 | 113 | (3.7) | |
| 14–27 | 73 | (2.4) | |
| ≥28 | 42 | (1.4) | |
| Treatment not started | 167 | (5.5) | |
| Transferred out of district (yes) | 521 | (17.3) | |
| Factors * | Total | Screened (Yes) | PR | (95%CI) | aPR ** | (95%CI) | ||
|---|---|---|---|---|---|---|---|---|
| n | (%) | |||||||
| Total | 3020 | 1531 | (50.7) | |||||
| Age in years | ||||||||
| 15–24 | 476 | 234 | (49.2) | Ref | # | |||
| 25–34 | 611 | 305 | (49.9) | 1.02 | (0.90, 1.15) | |||
| 35–44 | 619 | 321 | (51.9) | 1.05 | (0.94, 1.19) | |||
| 45–54 | 575 | 290 | (50.4) | 1.03 | (0.91, 1.16) | |||
| 55–64 | 416 | 207 | (49.8) | 1.01 | (0.89, 1.16) | |||
| ≥65 | 323 | 174 | (53.9) | 1.10 | (0.96, 1.26) | |||
| Gender | ||||||||
| Men | 2039 | 1045 | (51.3) | Ref | # | |||
| Women | 981 | 486 | (49.5) | 0.97 | (0.90, 1.04) | |||
| Test used for diagnosis | ||||||||
| Rapid molecular tests | 1630 | 789 | (48.4) | Ref | Ref | |||
| Microscopy/Culture | 566 | 294 | (51.9) | 1.07 | (0.98, 1.18) | 1.07 | (0.97, 1.18) | |
| Chest Radiograph | 272 | 168 | (61.8) | 1.28 | (1.15, 1.42) ^ | 1.09 | (0.98, 1.20) | |
| Others | 552 | 280 | (50.7) | 1.05 | (0.95, 1.15) | 1.16 | (1.05, 1.27) ^ | |
| Bacteriological confirmation | ||||||||
| Yes | 2284 | 1135 | (49.7) | Ref | # | |||
| No | 736 | 396 | (53.8) | 1.08 | (1.00, 1.17) | |||
| Site of TB | ||||||||
| Pulmonary | 2186 | 1210 | (55.4) | Ref | & | |||
| Extrapulmonary | 667 | 318 | (47.4) | 0.86 | (0.79, 0.94) ^ | |||
| Missing | 167 | 3 | (1.8) | 0.03 | (0.01, 0.10) ^ | |||
| Previous treatment | ||||||||
| Yes | 474 | 248 | (52.3) | 1.04 | (0.94, 1.14) | # | ||
| No | 2546 | 1283 | (50.4) | Ref | ||||
| HIV | ||||||||
| Positive | 225 | 109 | (48.4) | 0.90 | (0.79, 1.04) | 0.86 | (0.76, 0.98) ^ | |
| Negative | 2531 | 1358 | (53.7) | Ref | ||||
| Unknown | 264 | 64 | (24.2) | 0.45 | (0.36, 0.56) ^ | 0.85 | (0.69, 1.05) | |
| DM | ||||||||
| Positive | 505 | 274 | (54.3) | 0.99 | (0.91, 1.09) | 0.99 | (0.91, 1.07) | |
| Negative | 2086 | 1138 | (54.6) | Ref | ||||
| Unknown | 429 | 119 | (27.7) | 0.51 | (0.43, 0.60) ^ | 0.82 | (0.71, 0.95) ^ | |
| Bank details available | ||||||||
| Yes | 2353 | 1281 | (54.4) | Ref | ||||
| No | 667 | 250 | (37.5) | 0.69 | (0.62, 0.76) ^ | 0.87 | (0.79, 0.95) ^ | |
| Peripheral Health Institute—Notification facility | ||||||||
| District/Teaching hospital | 1942 | 847 | (43.6) | 0.65 | (0.60, 0.70) ^ | 0.87 | (0.81, 0.94) ^ | |
| Sub-district level hospital | 769 | 517 | (67.2) | Ref | ||||
| Primary health Centre | 206 | 100 | (48.5) | 0.72 | (0.62, 0.84) ^ | 1.11 | (0.95, 1.29) | |
| Days to notify from diagnosis | ||||||||
| Within a day | 2160 | 1098 | (50.8) | Ref | ||||
| 1–6 day | 632 | 352 | (55.7) | 1.10 | (1.01, 1.19) ^ | 1.07 | (0.99, 1.16) | |
| 7–13 | 113 | 54 | (47.8) | 0.94 | (0.77, 1.14) | 0.98 | (0.82, 1.18) | |
| 14–27 | 73 | 22 | (30.1) | 0.59 | (0.42, 0.84) ^ | 0.71 | (0.52, 0.98) ^ | |
| ≥28 | 42 | 5 | (11.9) | 0.23 | (0.10, 0.53) ^ | 0.31 | (0.14, 0.68) ^ | |
| Treatment started | ||||||||
| Yes | 2853 | 1528 | (53.6) | Ref | ||||
| No | 167 | 3 | (1.8) | 0.03 | (0.01, 0.10) ^ | 0.04 | (0.01, 0.17) ^ | |
| Transferred out of district | ||||||||
| Yes | 521 | 156 | (29.9) | 0.54 | (0.47, 0.62) ^ | 0.70 | (0.62, 0.80) ^ | |
| No | 2499 | 1375 | (55.0) | Ref | ||||
| Total Screened | ||
|---|---|---|
| n | (%) | |
| Total | 1531 | (100.0) |
| Data on all indicators collected | 1354 | (88.4) |
| Illegal entry or missing weight or height (missing BM) | 7 | (0.5) |
| Errors in BMI calculation | 126 | (8.3) |
| Instances where BMI ≤ 14.0 and able to stand without support | 133 | (8.7) |
| Missing details on leg swelling | 0 | (0) |
| Missing details on respiratory rate | 99 | (6.5) |
| Missing details on oxygen saturation | 88 | (5.7) |
| Missing details on ability to stand without support | 0 | (0) |
| Total | Men | Women | |||||
|---|---|---|---|---|---|---|---|
| Characteristics | n | (%) | n | (%) | n | (%) | |
| Total | 1531 | (100.0) | 1045 | (100.0) | 486 | (100.0) | |
| Weight (kg) | |||||||
| <30 | 33 | (2.2) | 9 | (0.9) | 24 | (4.9) | |
| 30–44 | 594 | (38.8) | 357 | (34.2) | 237 | (48.8) | |
| 45–59 | 674 | (44.0) | 516 | (49.4) | 158 | (32.5) | |
| ≥60 | 223 | (14.6) | 160 | (15.3) | 63 | (13.0) | |
| Missing | 7 | (0.5) | 3 | (0.3) | 4 | (0.8) | |
| Mean (SD) | 47.8 | (11.9) | 49.1 | (11.4) | 45.0 | (12.4) | |
| Body mass index (kg/m2) | |||||||
| ≤14.0 | 169 | (11.0) | 106 | (10.1) | 63 | (13.0) | |
| 14.1–16.0 | 288 | (18.8) | 198 | (18.9) | 90 | (18.5) | |
| 16.1–18.4 | 379 | (24.8) | 273 | (26.1) | 106 | (21.8) | |
| ≥18.5 $ | 688 | (44.9) | 465 | (44.5) | 223 | (45.9) | |
| Missing | 7 | (0.5) | 3 | (0.3) | 4 | (0.8) | |
| Mean (SD) | 18.7 | (4.4) | 18.5 | (4.1) | 19.0 | (5.1) | |
| Respiratory rate per minute | |||||||
| <18 | 240 | (15.7) | 158 | (15.1) | 82 | (16.9) | |
| 18–24 | 959 | (62.6) | 655 | (62.7) | 304 | (62.6) | |
| 25–30 | 120 | (7.8) | 77 | (7.4) | 43 | (8.8) | |
| >30 | 113 | (7.4) | 86 | (8.2) | 27 | (5.6) | |
| Missing | 99 | (6.5) | 69 | (6.6) | 30 | (6.2) | |
| Oxygen saturation (%) | |||||||
| ≥94 | 1288 | (84.1) | 870 | (83.3) | 418 | (86.0) | |
| 90–93 | 123 | (8.0) | 88 | (8.4) | 35 | (7.2) | |
| 85-89 | 14 | (0.9) | 12 | (1.1) | 2 | (0.4) | |
| <85 | 18 | (1.2) | 15 | (1.4) | 3 | (0.6) | |
| Missing | 88 | (5.7) | 60 | (5.7) | 28 | (5.8) | |
| Criteria | n | % | (95% CI) |
|---|---|---|---|
| Using the screening criteria | 538 | 35.1 | (32.8, 37.6) |
| Using BMI ≤ 14 | 169 | 11.0 | (9.6, 12.7) |
| Using BMI 14–16 with leg swelling | 15 | 1.0 | (0.6, 1.6) |
| Using RR > 24/min | 233 | 15.2 | (13.5, 17.1) |
| Using oxygen saturation < 94% | 155 | 10.1 | (8.7, 11.7) |
| Inability to stand without support | 148 | 9.7 | (8.3, 11.2) |
| Very severe undernutrition related indicator (any one) | 184 | 12.0 | (10.5, 13.7) |
| Respiratory insufficiency related indicator (any one) | 346 | 22.6 | (20.6, 24.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shewade, H.D.; Nagaraja, S.B.; Murthy, H.J.D.; Vanitha, B.; Bhargava, M.; Singarajipura, A.; Shastri, S.G.; Reddy, R.C.; Kumar, A.M.V.; Bhargava, A. Screening People with Tuberculosis for High Risk of Severe Illness at Notification: Programmatic Experience from Karnataka, India. Trop. Med. Infect. Dis. 2021, 6, 102. https://doi.org/10.3390/tropicalmed6020102
Shewade HD, Nagaraja SB, Murthy HJD, Vanitha B, Bhargava M, Singarajipura A, Shastri SG, Reddy RC, Kumar AMV, Bhargava A. Screening People with Tuberculosis for High Risk of Severe Illness at Notification: Programmatic Experience from Karnataka, India. Tropical Medicine and Infectious Disease. 2021; 6(2):102. https://doi.org/10.3390/tropicalmed6020102
Chicago/Turabian StyleShewade, Hemant Deepak, Sharath Burugina Nagaraja, Hosadurga Jagadish Deepak Murthy, Basavarajachar Vanitha, Madhavi Bhargava, Anil Singarajipura, Suresh G. Shastri, Ramesh Chandra Reddy, Ajay M. V. Kumar, and Anurag Bhargava. 2021. "Screening People with Tuberculosis for High Risk of Severe Illness at Notification: Programmatic Experience from Karnataka, India" Tropical Medicine and Infectious Disease 6, no. 2: 102. https://doi.org/10.3390/tropicalmed6020102