


ABSTRACT
Introduction:
Over the past 5 years, substantial global investment has resulted in reduced TB incidence rates by 9% and mortality rates by 14%. However, the coronavirus disease (COVID-19) pandemic has hindered access and availability of TB services to maintain robust TB control. The objective of this rapid review was to describe the challenges to be addressed and recommendations to strengthen health system preparedness for optimal TB control across low- and middle-income countries during and after the COVID-19 pandemic.
Methods:
Five databases were used to systematically search for relevant articles published in 2020. The 5-step framework proposed by Arskey and O'Malley and adapted by Levac et al. guided the review process. Thematic analysis with grounded theory principles was used to summarize themes from selected articles and integrate analyses with barriers reported from authors' previous TB research.
Results:
Of the 218 peer-reviewed articles, 20 articles met the inclusion criteria. Four emerging themes described challenges: (1) unprepared health system leadership and infrastructure, (2) coexisting health priorities, (3) insufficient health care workforce support for continued training and appropriate workplace environments, and (4) weak connections to primary health centers hindering community engagement. Four recommendations were highlighted: (1) ensuring leadership and governance for sustainable national health budgets, (2) building networks of community stakeholders, (3) supporting health care workforce training and safe workplace environments, and (4) using digital health interventions for TB care.
Conclusions:
National health systems must promote patient-centered TB care, implement ethical community interventions, support operational research, and integrate appropriate eHealth applications. TB program managers and primary care practitioners can serve as instrumental leaders and patient advocates to deliver high-quality and sustainable TB care that leads to achieving the targets of the End TB Strategy.
INTRODUCTION
Of respiratory infections, TB is the leading cause of global morbidity and mortality, causing 10 million new TB cases and 1.4 million TB deaths in 2019.1 TB is spread through aerosol droplets, including those smaller than 5 microns, infected with M. tuberculosis from an infected individual to a susceptible individual. One-third of the global population, which is estimated to have an asymptomatic M. tuberculosis infection, has a 5%–10% risk of developing TB disease during their lifespan.2 With substantial global investment and political commitment over the past 5 years, TB incidence and mortality rates have continued to decrease by 9% and 14%, respectively.1 To minimize disease transmission, strict adherence to evidence-based infection control and prevention measures are recommended in clinical and community settings.3
The End TB Strategy has set ambitious milestones for 2025 and targets to end TB by 2035.4 Three pillars place precedence on expanding patient-centered TB prevention and control efforts, forming policies and multisector collaborations across communities and public and private sectors, and ensuring continued attention on scientific research innovations for TB care.4 However, these robust efforts have been redirected to support the coronavirus disease (COVID-19) response measures. Economic and human resources for health have been diverted to emergency care and contact tracing of COVID-19 patients, and laboratories have been repurposed for COVID-19 diagnostic testing.5 As a result, health care services for infectious diseases and comorbidities of significant burden—like TB, HIV/AIDS, and malaria—diminished,5 and citizens were fearful to seek TB diagnostic and treatment services.6 During the Ebola virus disease outbreak in West Africa in 2014–2015, similar observations were reported, such as reductions in TB, HIV, and malaria case notifications and treatment, reductions in health care utilization including vaccination coverage, and the breakdown of community cohesion due to fear, apprehension, and socioeconomic impacts.7–9
Health systems should recognize the syndemic effects of TB and COVID-19 and analyze 3 factors for best clinical and community management practices of competing health priorities. First, the social determinants of health draw attention to the impact of social environments (e.g., education and income), physical environments (e.g., residence and transportation), and access and quality of health care services, including access to broadband internet.10,11 Second, the One Health concept promotes the development of multidisciplinary collaborations to advance clinical and research applications focusing on the human-animal-environment nexus.12,13 Third, the “knowledge-action” gap can result from limitations in the access of up-to-date scientific knowledge (e.g., health care professions curricula and continuing education), health system infrastructure (e.g., financial resources and surveillance programs), and social environments (e.g., access to health care services and influence of news sources).14,15 Hence, the primary health care workforce can contribute to public debates and community campaigns, develop patient education materials on pressing health issues,16 and lead efforts to implement evidence-based findings that can optimize clinical, educational, and research practices related to TB care.
Health systems should recognize the syndemic effects of TB and COVID-19 and analyze 3 factors for best clinical and community management practices of competing health priorities.
To date, numerous countries have reported reduced TB case notifications during the COVID-19 pandemic, reflecting the importance of “The Clock is Ticking” theme for World TB Day 2021.17,18 Over the next 5 years, modeling estimates depict that countries with high TB burden will report up to 20% increased TB mortality or 1.4 million TB deaths,17,19 which will negatively impact the End TB Strategy timeline.20 In this article, we summarize encountered challenges to be addressed and proposed recommendations from the literature that can strengthen TB prevention and control efforts during and after the COVID-19 pandemic. Moving forward, national health systems can integrate these recommendations into future practices and policies that strengthen health care service delivery, health care professions education, and research capacity related to TB care.
METHODS
A rapid review was conducted to review the current literature, identify gaps, and synthesize findings,21,22 related to challenges and recommendations for TB prevention and control in low- and middle-income countries. We used the 5-step framework proposed by Levac et al.,23 which was adapted from Arksey and O'Malley,24 in our search strategy: (1) identify the research question; (2) identify relevant studies; (3) select studies, (4) chart the data; and (5) collate, summarize, and report the results.23,24 The research questions were: (1) What are the existing challenges in TB prevention and control efforts during the COVID-19 pandemic? and (2) What are the proposed recommendations that can strengthen TB prevention and control efforts during and after the COVID-19 pandemic? This search was simultaneously integrated with findings reported from a previous qualitative study that examined challenges in TB prevention and control in a middle-income country, the Dominican Republic.25–27
Search Strategy and Selection Criteria
On January 10, 2021, 2 authors (HJC, BAV) searched 5 databases (PubMed, Scopus, Web of Science, EBSCO Academic Search Premier, SciELO Citation Index). They used the terms “COVID-19,” “coronavirus,” “health systems,” and “tuberculosis,” to include original articles, reviews, commentaries, and letters, published between January 1, 2020, and December 31, 2020. After removing duplicate articles, authors independently reviewed each abstract and included articles that described the impacts of TB control efforts during the COVID-19 pandemic and proposed recommendations to strengthen health system efforts for TB control. If any disagreement occurred, authors discussed the abstract until consensus was finalized. Articles written in languages other than English were not excluded.
Articles were excluded if they did not include content related to TB and COVID-19, if clinical aspects of TB and COVID-19 management were described or if the focus deviated from the impact of COVID-19 on TB prevention and control efforts of the health system. Authors incorporated relevant citations from selected articles in the analysis. The article screening and selection process is shown in Figure 1.

Article Selection Process for a Rapid Review on TB Control Efforts During and After the COVID-19 Pandemic
Data Extraction and Analysis
After full-text review, authors used the matrix method, with paper trail, documents, review matrix, and synthesis folders, to extract data from each article.28 Data included the country or continent focus, study objective, and main summary points related to challenges to overcome and recommendations for TB prevention and control.
After compiling this information, authors used a qualitative thematic analysis applying grounded theory principles29 to identify themes or patterns from selected articles and explore the connections between existing challenges and proposed recommendations to improve TB prevention and control. The 6-step approach of Braun and Clarke30 guided the analysis, where authors expanded upon the final themes identified from previous TB research to examine health care workers' perceived barriers to adherence to TB prevention measures in the Dominican Republic.25–27 Authors independently reviewed the initial codes and extracted information to support and expand their meaning. They jointly reviewed and agreed on all final codes, compiled them into relevant themes, and developed a conceptual model.
RESULTS
The search yielded 218 articles, and after 58 duplicate articles were removed, 160 titles and abstracts were reviewed by both authors. Of the 160 articles, 19 articles met the inclusion criteria, and 1 additional article was added from the manual reference search of these articles. Of the 20 included articles, articles described the TB burden in Africa (n=8), Asia (n=2), and the world (n=10). Article types included 4 letters, 9 perspectives, 5 reviews, and 2 original research articles. Emerging themes from selected articles were identified as existing challenges to be addressed and proposed recommendations to strengthen TB prevention and control efforts (Figure 2).
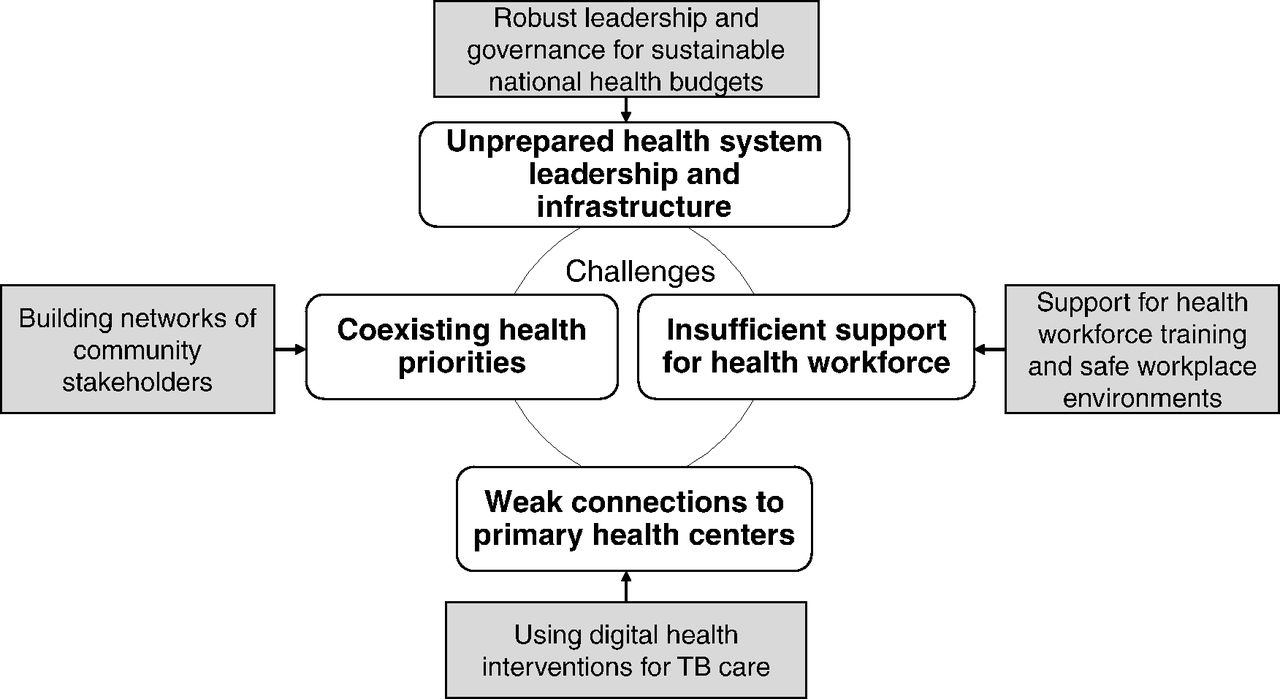
Conceptual Figure That Incorporates Recommendations to Mitigate Existing Challenges and Improve TB Control
The characteristics of each article, including proposed recommendations to strengthen TB control efforts during and after the COVID-19 pandemic, are shown (Table 1 and Supplement).
Selected Articles for the Rapid Review of Literature on Recommendations for TB Prevention and Control During the COVID-19 Pandemic in Low- and Middle-Income Countries
Existing Challenges in TB Prevention and Control
Four emerging themes on existing challenges in TB prevention and control efforts are displayed (Table 2).
Four Emerging Themes on Existing Challenges in TB Prevention and Control Efforts
An unprepared public health system leadership and infrastructure was described by limited short-term plans, inadequate funding for high-burden diseases, and limited foresight to identify key factors that hinder TB control efforts.
Coexisting health priorities were exacerbated with disruptions in routine TB care, limited understanding of how natural emergencies impact established health programs, and lack of oversight on the importance of TB programs.
Insufficient health care workforce support for continued training and appropriate workplace environments was impacted by the demanding schedules of health care workers and the need for reassigned roles to meet national requests.
Weak connections to primary health centers resulted in interrupted community-based programs that hindered patient-provider interactions on routine health care services and negatively impacted early diagnostics and adherence to management.
Coexisting health priorities were exacerbated with disruptions in routine TB care, limited understanding of how natural emergencies impact established health programs, and lack of oversight on the importance of TB programs.
Proposed Recommendations to Strengthen TB Prevention and Control Efforts
Emerging themes on proposed recommendations to strengthen TB prevention and control efforts are listed (Table 3).
Four Emerging Themes on Recommendations to Strengthen TB Prevention and Control Efforts
Ensuring Leadership and Governance for Sustainable National Health Budgets
With the risk of national emergency scenarios—whether natural disasters, infectious disease outbreaks, or conflict—nations should implement policies and strategies and allocate funding that strengthens prevention and mitigation efforts for infectious and chronic diseases.48,52,53 Political commitment is essential to support core health care services that sustain high-quality point-of-care diagnostics and treatment plans for TB patients as well as balancing these needs with the coexisting pandemic.19,37,41–43 These actions can focus on long-term and comprehensive care for TB and coexisting priorities like COVID-19.6,32,36,45
Following the World Health Organization's call that all nations should conduct and utilize research capacity, researchers can investigate key scientific questions raised during coinciding pandemics.37,41,46 For example, operational research should be conducted to examine the influence of social determinants of health on TB and COVID-19, vaccine effectiveness and community acceptability, and adherence to recommended pharmaceutical regimens.39,40,45,50 These research findings can inform national health priorities, which can provide a framework for the appropriate allocation of economic resources. Supported by appropriate legislature, authorities can recommend actions for the health sector to best distribute resources for current health priorities and unanticipated emergency scenarios.50
Building Networks of Stakeholders to Sustain Community Resources
Forming a network of stakeholders—or community groups comprised of individuals who represent different disciplines but share common goals51—can help identify community needs and health system vulnerabilities related to TB prevention and control. As community stakeholders share approaches and lessons learned, a multisectoral response that aims to reduce TB burden can drive community engagement with families6,31,43,49 and support health care workers in facilitating educational activities as a platform to increase TB awareness and reduce stigma.41,45 By working with community stakeholders, health leaders can identify high-risk communities of poor health status, including inadequate nutrition, overcrowded living conditions, and unemployment, and advocate for creative solutions to improve public welfare programs.34,35,38 These programs can drive national action to offer social protection for TB patients, such as cash transfers or food parcels, and essential psychosocial support.45
Coupled with these health promotion activities, community-based research can highlight the use of key epidemiology tools and trends to better understand the transmission of emerging diseases like COVID-19 and emphasize the existing syndemic and closely linked influencing factors like poverty.45 This insight can be applied to current and future plans of TB programs, especially for the diagnosis and management of active and reactivation TB cases.32 Health authorities can also streamline public health efforts in COVID-19 and TB control by minimizing duplicated or non-essential approaches and guiding simultaneous surveillance services for rapid response.37,49 By identifying potential funding partners in the public and private sectors, additional financial resources and equipment can be distributed to health facilities.31,44
Community-based research can highlight the use of key epidemiology tools and trends to better understand the transmission of emerging diseases like COVID-19 and emphasize the existing syndemic.
Supporting High-Quality Health care Workforce Training and Safe Workplace Environments
A competent health care workforce must be prepared with appropriate knowledge and skills to simultaneously manage endemic and emerging health threats. Health care workers should receive adequate training, appropriate incentives to provide care, and mental health and psychosocial support.36,41 Continuing education programs can offer up-to-date information about clinical guidelines, best practices, public health principles, and timely health topics.32 This information can offer insight on the influence of social determinants on TB and COVID-19 patients, especially the impact of co-morbidities (e.g., diabetes mellitus), environmental contamination (e.g., air pollution), and economic hardships (e.g., poverty and overcrowded living conditions), and strategies to reduce stigma and discrimination.6,45 Community fora can offer public platforms to share and discuss evidence-based findings that can promote a call to action for policy changes.49 These key contributions to health systems will support the delivery of holistic, patient-centered care services for TB patients.
Community fora can offer public platforms to share and discuss evidence-based findings that can promote a call to action for policy changes.
Health care workers should receive additional skills-based training in field epidemiology with case studies for outbreak investigations and operational research for TB prevention and control. This training can offer skills in identifying priority health issues, literature reviews, connecting with community stakeholders, data collection and analysis, and scientific writing.39,41,49 However, with increasing clinical and community health responsibilities—including allocation of staff and resources to new disease priorities—it is important to monitor and evaluate health care workers for mental health stressors and mitigate risk of burnout.39,41
Using Digital Health Interventions for TB Care
Existing electronic health technologies (eHealth), defined as platforms that use information and communication technologies,52 have the potential to change the paradigm in TB management. These digital innovations can offer remote support through video-supported therapy and electronic medication monitors for health care workers to guide TB patients through their clinical management, identify and monitor co-morbidities, and encourage treatment adherence.33,36,38,39 Mobile health solutions (mHealth) facilitate the delivery of short message service (SMS) and WhatsApp messages as well as geographic information systems (GIS) mapping for direct contact and delivery of test results and health information,39,47 especially reaching at-risk communities.33 With increased public interest observed during the COVID-19 pandemic, these digital approaches can enhance public engagement on infectious disease monitoring and offer informative fact sheets on multiple infectious diseases.39,44 These telemedicine applications, albeit with clear benefits for provider-patient engagement, raise potential questions for health care delivery. Some remaining issues include the ability to ensure patient safety, warrant data privacy and storage, conduct appropriate virtual physical exams, follow limited established protocols, evaluate cost-effectiveness, and assess adherence to improve overall equity and efficiency.41,43,45 Although comprehensive in-person evaluations cannot be eliminated from acute and chronic patient care,42 an integrated approach of in-person consultations and complementary telemedicine applications can pave the future for TB prevention and control efforts.
DISCUSSION
This is the first known rapid review to examine the existing challenges to be addressed and proposed recommendations to strengthen TB efforts in low- and middle-income countries during and after the COVID-19 pandemic. The End TB Strategy targets were approached in 2020, but not met, with established targets of 20% decrease in incidence rates (reported 9% decrease) and 35% decrease in mortality rates (reported 14% decrease), with continued challenges in the Americas and African regions.1,53,54 Increased attention to TB efforts will be fundamental in the upcoming years to combat the decreased TB notification rates reported during the COVID-19 pandemic; support national policies that prioritize integral, patient-centered TB care; and expand current initiatives to end TB transmission.53
Increased attention to TB efforts will be fundamental in the future to combat the decreased TB notification rates reported during the COVID-19 pandemic, support national policies that prioritize patient-centered TB care, and expand current initiatives to end TB transmission.
Since emerging One Health threats continue to affect the global society, health leaders must be innovative in their contributions to clinical and community settings. Global health systems must be vigilant and prepared to adapt current evidence-based practices to meet societal needs of the next decade.55 In this review, selected studies identified challenges in TB control efforts—such as overwhelmed health systems and insufficient support for the health care workforce—that will require novel solutions to improve access and availability of diagnostic and treatment services for TB patients. The use of ground-breaking approaches, data, and practices that can help identify specific challenges, such as country-specific social, economic, and cultural contexts that influence health-seeking behaviors and treatment adherence,35 should be considered in maintaining sustainable TB programs.
A robust national health system with skilled leadership, trained health care workforce, health system and research investment, and direct connections with community stakeholders has the potential to achieve the national and international objectives of the Sustainable Development Goals (SDG 3.3) and the End TB Strategy. Political commitment will enhance national preparedness and guarantee an immediate public health response, noting stressors (e.g., dual health priorities) to a well-functioning health system.56 Continued investment in operational TB research is essential to identify knowledge gaps, develop sophisticated scientific inquiries, establish methodological and analytical approaches, and implement findings in public health practice.54,57,58
Strengthening links with primary care centers and relevant community stakeholders will elucidate local needs and resources as well as knowledge gaps related to TB care. National programs that advocate for public welfare and social protection for TB patients, including cash transfers, food parcels, housing resources, and psychosocial support, can minimize existing inequities in TB care, alleviate additional psychological stress, and offer indispensable support to TB patients and their families.45,59 Partnerships that expand public sector engagement with the private sector (public-private mix) for TB care are essential to meet the targets of the End TB Strategy, including ensuring prompt TB diagnosis and treatment, reducing hardships associated with catastrophic health care costs, and ultimately curbing TB transmission.61,62 National health statistics from active surveillance programs provide data on population health risks to authorities for health decision-making activities. Through qualitative research designs, health researchers can capture barriers related to TB treatment adherence, primary care providers' perspectives on TB control, and social determinants of health.27,62,63 Further exploration of the role and acceptance of digital innovations to TB care can be examined among the health care workforce and community members.64
Supporting a highly trained health care workforce and safe workplace environments is the responsibility of national health systems, especially with the renewed emphasis on the public-private mix for TB care and prevention. Comprehensive training with required annual continuing education hours for the health care workforce across the public and private sector will reinforce robust technical capacity, offer uniformity across institutions, and expand reach to resource-limited areas.65 Appropriate incentives for health care workers, such as financial bonuses, professional recognition, and supervisory positions, have the potential to motivate self-confidence and morale in professional competencies as well as enhance work satisfaction and productivity.66 Without this support, the brain drain phenomenon can lead to significant health care workforce shortages as workers migrate to other countries that offer improved working conditions, higher salaries or incentives, personal security, and professional recognition.67 Supervisors can also provide mentorship and objective feedback, encouraging health care workers to reach specific milestones in their performance plan.68
Digital health interventions can transform TB care by disseminating essential health information, supporting treatment adherence, and encouraging health-seeking behaviors among TB patients. With increased interest and versatility among health professional students, social media platforms have been successfully used to expand health communication efforts during the Ebola virus disease outbreak in West Africa69 and guide One Health community field campaigns.70 It has the potential to combat the “infodemic”—defined as the rapid spread of false information—of TB and other stigma-associated diseases like COVID-1971 as well as streamline operational networks in the public-private mix approach.61 Furthermore, telemedicine applications have strengthened provider-patient engagement and TB diagnostic and treatment adherence through text messaging72 and computer-aided technology.73 Patient safety issues, however, should be evaluated, especially ensuring data security and storage, confirming internet connectivity and related infrastructure, and training health workers in remote technologies.43,73 Although the use of broadband internet can substantially enhance the innovative delivery of TB health care services and educational programs, national health systems should identify existing disparities in internet access that can further exacerbate the “digital divide” as a social determinant of health.11,74
Limitations
This study has a few limitations. First, although the authors participated in the data analysis and selected the final themes, they recognize that data may be interpreted in alternative ways.75 Second, the study utilized 5 databases for peer-reviewed articles but may have overlooked other relevant papers in the gray literature or other scientific databases. Finally, this study did not evaluate the quality of described challenges and recommendations of selected articles, although this task is not obligatory for rapid reviews.24 However, authors did critically analyze the study findings from original research articles and reviews with more substantial detail, than the letters and perspective articles.
CONCLUSION
This rapid review summarizes areas for improvement in health system preparedness for optimal TB control across low- and middle-income countries. These findings can aid in the development of national policies to promote integral, patient-centered TB care, facilitate the implementation of ethical community interventions, support operational research, and allow the integration of appropriate eHealth applications. By better understanding challenges in TB prevention and control with coexisting health priorities, TB program managers and primary care practitioners can serve as instrumental leaders and patient advocates to deliver high-quality and sustainable TB care that leads to achieving targets of the End TB Strategy.
Acknowledgments
The authors recognize the significant contributions of all health care workers, who are dedicated to clinical care, community health, education, health policy, laboratory diagnostics, and research, to combat infectious diseases like TB and COVID-19.
Disclaimer
The views expressed in this article are those of the authors and do not reflect the official policy or position of the George Washington University or the Universidad Católica del Cibao.
Author contributions
Chapman and Veras-Estévez had substantial contributions to the preparation and completion of the article drafts.
Competing interests
None declared.
Notes
Peer Reviewed
First published online: November 30, 2021.
Cite this article as: Chapman HJ, Veras-Estévez BA. Lessons learned during the COVID-19 pandemic to strengthen TB infection control: a rapid review. Glob Health Sci Pract. 2021;9(4):964-977. https://doi.org/10.9745/GHSP-D-21-00368
- Received: June 5, 2021.
- Accepted: September 14, 2021.
- Published: December 31, 2021.
- © Chapman and Veras-Estévez.
This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visit https://creativecommons.org/licenses/by/4.0/. When linking to this article, please use the following permanent link: https://doi.org/10.9745/GHSP-D-21-00368









{kind=link}
{kind=link}