


ABSTRACT
Health sector priorities and interventions to prevent and manage noncommunicable diseases and injuries (NCDIs) in low- and lower-middle-income countries (LLMICs) have primarily adopted elements of the World Health Organization Global Action Plan for NCDs 2013–2020. However, there have been limited efforts in LLMICs to prioritize among conditions and health-sector interventions for NCDIs based on local epidemiology and contextually relevant risk factors or that incorporate the equitable distribution of health outcomes. The Lancet Commission on Reframing Noncommunicable Diseases and Injuries for the Poorest Billion supported national NCDI Poverty Commissions to define local NCDI epidemiology, determine an expanded set of priority NCDI conditions, and recommend cost-effective, equitable health-sector interventions. Fifteen national commissions and 1 state-level commission were established from 2016–2019. Six commissions completed the prioritization exercise and selected an average of 25 NCDI conditions; 15 conditions were selected by all commissions, including asthma, breast cancer, cervical cancer, diabetes mellitus type 1 and 2, epilepsy, hypertensive heart disease, intracerebral hemorrhage, ischemic heart disease, ischemic stroke, major depressive disorder, motor vehicle road injuries, rheumatic heart disease, sickle cell disorders, and subarachnoid hemorrhage. The commissions prioritized an average of 35 health-sector interventions based on cost-effectiveness, financial risk protection, and equity-enhancing rankings. The prioritized interventions were estimated to cost an additional US$4.70–US$13.70 per capita or approximately 9.7%–35.6% of current total health expenditure (0.6%–4.0% of current gross domestic product). Semistructured surveys and qualitative interviews of commission representatives demonstrated positive outcomes in several thematic areas, including understanding NCDIs of poverty, informing national planning and implementation of NCDI health-sector interventions, and improving governance and coordination for NCDIs. Overall, national NCDI Poverty Commissions provided a platform for evidence-based, locally driven determination of priorities within NCDIs.
BACKGROUND
Noncommunicable diseases and injuries (NCDIs) are a major contributor to morbidity and mortality in low- and lower-middle-income countries (LLMICs).1 The World Health Organization (WHO) Global Action Plan for Prevention and Control of Noncommunicable Diseases (NCDs) 2013–2020 emphasizes 4 behavioral risk factors (tobacco use, unhealthy diets, physical inactivity, and harmful use of alcohol) in the context of 4 disease groups (cardiovascular diseases, diabetes, cancer, and chronic respiratory diseases), subsequently expanded to include air pollution and mental health disorders.2,3 However, there is increasing evidence that this framework does not adequately represent the diverse and comprehensive set of risk factors and NCDIs comprising the disease burden in LLMICs.4,5 The conditions comprising this burden in resource-constrained settings are diverse, and infectious diseases and conditions related to poverty comprise a large component of associated risk factors.6,7 These conditions not only result in a large burden of disease in LLMICs, but due to younger population demographics, delays to diagnosis, and limited service availability, they tend to occur earlier and more severely in these populations.8 Prolonged chronicity of these conditions along with dependency on out-of-pocket payments for NCDI services result in dramatic impoverishment and productivity losses as compared to other disease areas.9,10
To date, NCDI strategic plans and frameworks in LLMICs have been largely influenced by elements of the existing global action plan and monitoring framework.11 Efforts to adapt or contextualize the WHO Global Action Plan for Prevention and Control of NCDs to the national burden of NCDI conditions or health system capacities in LLMICs have been inadequately prioritized or resourced.11–13 Interventions proposed to avert the burden of NCDIs have focused on primary and secondary prevention of conditions due to behaviorally mediated risk factors and have not frequently considered a broader range of NCDIs and their associated risk factors.11 Furthermore, these interventions have been largely evaluated and selected based on measures of cost-effectiveness and feasibility within resource-constrained environments and have not traditionally included measurements of equitable distribution of health outcomes at country-level.14
Efforts to adapt or contextualize the WHO Global Action Plan for Prevention and Control of NCDs to the national burden of NCDI conditions or health system capacities in LLMICs have been inadequately prioritized or resourced.
The Lancet Commission on Reframing Noncommunicable Diseases and Injuries for the Poorest Billion (“Lancet NCDI Poverty Commission”) was established to assess the nature of the NCDI burden among the poorest billion people in the world, assure that sustainable financing is not a bottleneck to NCDI prevention and treatment among the world’s poorest, and expand the NCD movement and the global health agenda to urgently address NCDIs among the poorest billion.5 The Lancet NCDI Poverty Commission additionally aimed to work with stakeholders in a diverse group of countries to develop actionable pro-poor pathways for expansion of NCDIs interventions. To achieve these objectives, the Lancet NCDI Poverty Commission established and supported national and subnational NCDI Poverty Commissions in countries with high rates of extreme poverty.
In this article, we first describe the structure and analytic framework used by the national NCDI Poverty Commissions (termed “commissions”). We then provide a synthesis of the characteristics, findings, and recommendations reported by the commissions. Lastly, we report results of a semistructured survey and qualitative interviews conducted with key informants from the commissions regarding short-term outcomes of the commissions in 11 thematic areas corresponding to major objectives of the Lancet NCDI Poverty Commission framework.
METHODS
Commission Establishment and Capacity Building
The Lancet NCDI Poverty Commission was established in 2015 and supported administratively and technically by a central secretariat at the Program in Global NCDs and Social Change at Harvard Medical School. The measure used by the Lancet NCDI Poverty Commission to assess poverty was a global multidimensional poverty index based on indicators of living standards and education obtained through routine and standardized household surveys.15,16 The “poorest billion” were defined as households with deprivations in at least 5 of the 8 indicators included in this modified index.
Key individuals active in clinical, research, programmatic, or governance aspects of the NCDI health sector response from a diverse representation of this group of countries were invited to review the analytic framework developed for the Lancet NCDI Poverty Commission and propose adaptations to reflect national objectives (detailed in Analytic Approach). The Lancet NCDI Poverty Commission then invited the Ministry of Health of each key informant’s respective country to formally nominate and commission a national group of multisectoral experts in NCDIs to undertake an analytic and consultative process with technical, financial, and administrative support from the Lancet NCDI Poverty Commission secretariat.
From January to December 2016, 10 countries were invited to apply for support to establish an NCDI Poverty Commission (Round I). Five additional countries and 1 subnational region (Chhattisgarh State, India) were invited to establish commissions from October 2018 to September 2019 (Round II). Each Ministry of Health nominated 1 to 2 chairpersons to lead the commission, a coordinator to administer commission activities and communications, and approximately 20–30 multisectoral experts in the area of NCDIs, including policy makers, clinicians, researchers, patient group advocates, health economists, and health-sector planning experts.
All national commissioners were invited to participate in a series of 6 online “Knowledge Exchange” teleconferences jointly organized by the Lancet NCDI Poverty Commission and the World Bank. These teleconferences consisted of didactic presentations from global experts and participatory discussions facilitated by commission leads.17 Subregional meetings in East Africa (Kigali, Rwanda, March 2018) and Southern Africa (Maputo, Mozambique, June 2018) and a 4-day workshop entitled “The NCDI Poverty Commission Initiators’ Workshop” (Dubai, United Arab Emirates, 2018) were held to foster collaboration and knowledge sharing among commissions.18
Analytic Approach by Commissions
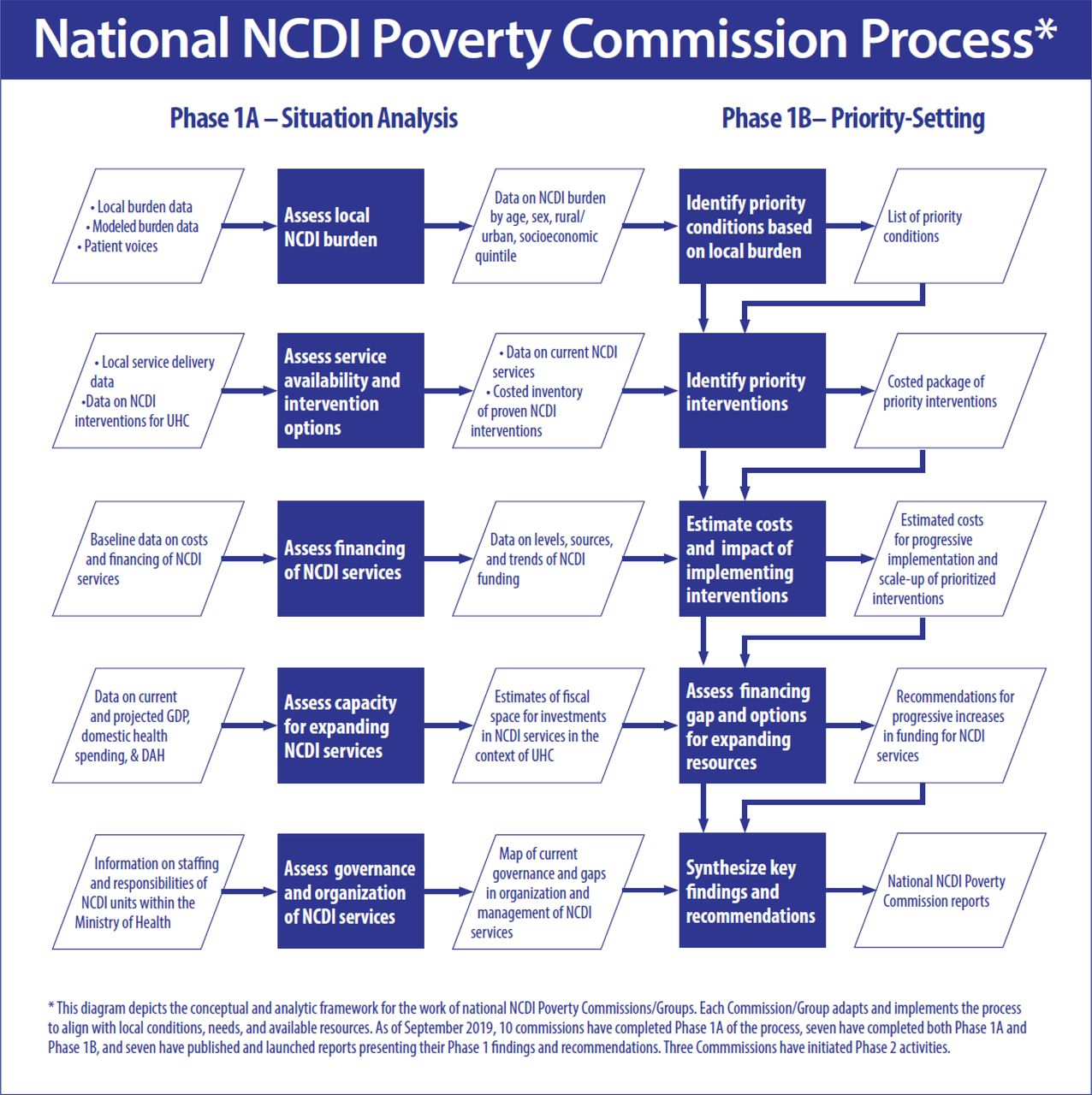
An analytic framework to achieve national commission objectives was developed (Figure 1). Phase 1A focused on aggregating a range of available data related to the burden of disease, service availability, financing, and governance of NCDI services in each country (Supplement Table 1). Descriptive statistics regarding population demographics were obtained from the Global Burden of Disease study (GBD) 2017 and World Bank World Development Indicators.1,19 Data regarding health expenditures were obtained from national health accounts compiled and available from the WHO Global Health Expenditure Database and human resources from the WHO Global Health Workforce Statistics.20,21

National Noncommunicable Diseases and Injuries Poverty Commission Analytic Framework
Abbreviations: DAH; developmental assistance for health; GDP, gross domestic product; NCDI, noncommunicable diseases and injuries; UHC, universal health coverage.
In Phase 1B, national commissions convened a set of deliberations and meetings to review the available evidence in NCDIs and make recommendations for local policy. This prioritization exercise was structured using the principles of priority setting established by the WHO Consultative Group on Equity and Universal Health Coverage.22 To develop a list of priority NCDI conditions, the commissions analyzed and ranked NCDI conditions in several dimensions, including the burden of disease, severity, and disability, using data from the GBD study.23 The overall burden of disease of each condition at the national level was measured by disability-adjusted life-years (DALYs). Severity was calculated using the average years of life lost (YLLs) per death, and disability was calculated by years lived with disability (YLDs) per prevalent case. The age-standardized DALY rate per 100,000 population was compared for each condition to high-income country rates as a reference standard. A total of 190 NCDI conditions from the GBD database were analyzed using these 4 metrics, and a summary score was provided to each condition according to an average of the ranking quartiles. Each of the 4 metrics was weighted according to its relative importance as determined by each commission. The 50 conditions with the highest priority summary scores were then reviewed by a subcommittee of the national commission. Commissioners then selected conditions that they believed (1) contribute significantly to adverse health and economic consequences in their respective country, (2) could be feasibly and effectively controlled in their local context, and (3) were aligned with or complementary to existing national policies and strategic plans.
Information regarding evidence-based and cost-effective health-sector interventions was obtained from the Disease Control Priorities Project, which produced model lists of essential health-sector interventions and essential intersectoral health policies for the Disease Control Priorities, 3rd Edition (DCP3) publication. DCP3 recommended 21 packages consisting of a total of 218 health-sector interventions to achieve essential universal health coverage (EUHC) in LLMICs based on key intervention metrics, including cost-effectiveness, financial risk protection, and equity scores (Supplement Table 2).24 The 65 interventions pertaining to NCDI conditions recommended as part of EUHC were reviewed by the national commissioners and evaluated for (1) alignment with stated NCDI priority conditions; (2) feasibility and desirability in the national context, and (3) cost-effectiveness, financial risk protection, and equity scores as assessed by DCP3.25 Commissions conducted customized deliberative processes to select a final set of interventions. Several commissions also considered additional interventions suggested by commissioners using locally available data (not included in costing estimates). In Ethiopia, the commission considered an expanded set of 235 interventions consisting of DCP3-recommended interventions as well as locally customized interventions.26
The commissions estimated the costs of their recommended interventions using methods and data that built on the cost modeling done for DCP3.27 In brief, costs were estimated as a function of: (1) the number of beneficiaries requiring each intervention (derived from GBD incidence, prevalence, or population estimates); (2) unit costs for each intervention (derived from published literature and extrapolated to different countries based on variation in labor and capital costs); and (3) proportion of the population “covered” by the intervention. Each intervention was assigned a current coverage, estimated from existing data sources or expert opinion (from the commissioners) if local data were not available. The commissions then assigned a feasible target coverage for each intervention within a timeframe of 5 to 10 years. Finally, the total annual cost of implementing each intervention at the additional coverage increment was calculated as the product of (1), (2), and (3). The commission in Ethiopia used an alternative method to estimate the cost of prioritized recommendations based on bottom-up costing through the use of the One Health tool, described in greater detail elsewhere.26
In each country, findings and recommendations were synthesized and disseminated to national stakeholders. The target audience for commission recommendations included government officials (national and subnational level), clinical leaders, implementation partners, donors, patient advocacy groups, local media, and the general public. Dissemination occurred through the publication of findings and recommendations, public launch events, media coverage, social media, advocacy meetings, and the NCDI Poverty website (Supplement Table 1). To further enhance awareness and local understanding of these conditions, commissions were additionally invited to develop video documentary narratives of young individuals living with severe NCDIs in populations of extreme poverty. Patients were selected for the documentary narratives as determined by each commission.
Design and Methodology of Evaluation
From April to November 2019, the Lancet NCDI Poverty Commission Secretariat conducted a 2-part evaluation to understand how commissions influenced national-level dialogue and policies. This evaluation consisted of a semistructured online survey and phone-based qualitative interview. Each of the commissions in Round I was invited to nominate a key informant (generally a commission chair or coordinator) to complete the online survey. Respondents were asked a series of open-ended questions related to their respective commission’s work in 11 thematic areas corresponding to major objectives of the Lancet NCDI Poverty Commission framework.5 The survey was administered through the Qualtrics platform without time limitation. Respondents were encouraged to consult with other members of their national commissions in developing their responses to the online survey.
After completing the online survey, respondents were invited to participate in a follow-up interview in which the respondent could provide in-depth, detailed elaborations on survey responses.
Online and interview responses were entered into Dedoose version 8.3.35. Each transcript was coded independently by the 2 researchers. The number of respondents reporting positive outcomes on the online survey or interview was tabulated by thematic area.
The online survey and qualitative interviews were approved by the Harvard University Longwood Medical Area Institutional Review Board. All participants were provided a standardized consent form and asked to provide consent before beginning the data collection. Consent was provided electronically for the online survey and verbally for the interviews.
RESULTS
Commission Countries and Characteristics
In Round I, commissions were established in 9 countries including Afghanistan, Ethiopia, Haiti, Kenya, Liberia, Malawi, Mozambique, Nepal, and Tanzania (Table 1). In Rwanda, a research group was formed to undertake this analysis rather than a formal commission. In Round II, commissions were established in an additional 5 countries including Madagascar, Sierra Leone, Uganda, Zambia, and Zimbabwe, and 1 subnational region (Chhattisgarh State, India). Two countries (Rwanda and Zambia) opted to not use the nomenclature of “commission” formally and instead used the terms “group” and “task force”, respectively. Although formally established, the commission in Madagascar had not yet begun activities as of July 2020. Twenty-two individuals were nominated as commissioners or official group participants for each commission. As of July 2020, 7 commissions had completed the prioritization exercise and cost estimation analysis (Phase 1B) and an additional 5 commissions were in the process of completing this analysis. Additionally, 80 patient narratives were developed in video documentary format across 5 countries representing a range of NCDI conditions, including type I diabetes, rheumatic heart disease, chronic kidney disease, breast cancer, cervical cancer, neuroblastoma, childhood leukemia, schizophrenia, and disability due to traumatic injury.28
Key Characteristics of States and Countries With Established National Noncommunicable Diseases and Injuries Poverty Commissions
Commissions’ Findings of NCDI Burden of Disease and Expenditure (Phase 1a)
On average across the 16 countries and states, 45.2% of DALYs were attributed to NCDIs (range 33.5–68.6%; Table 2), and 55.1% of DALYs due to NCDIs occurred before age 40 years (range: 36.4–62.9%). Additionally, 60.2% of the NCD DALYs across this group of countries were associated with NCD conditions other than those comprising the 4 disease categories included in the global NCD action plan (cardiovascular diseases, chronic respiratory diseases, diabetes, and cancer). When considering an expanded “5 by 5” framework that includes mental health and substance use disorders, 49.2% of NCD DALYs were from other conditions. In terms of injuries, 73.7% of DALYs due to injuries across this set of countries were due to injuries other than road traffic injuries (data not shown here).
Baseline National NCDI Poverty Commission Findings on the Proportion, Severity, Diversity, and Expenditure on NCDIsa
Across 16 countries and states, 60.2% of the NCD DALYs were associated with NCD conditions other than those comprising the 4 disease categories in the global NCD action plan.
Ten of the 15 countries (not including Chhattisgarh state) had available estimates for domestic government and external expenditures for NCDs and injuries. In these countries, the proportion of government health expenditure for NCDIs as a proportion of general government health expenditures ranged considerably, from 4.3%–50.5% for NCDs and 1.1%–8.9% for injuries. The proportion of external expenditures was consistently lower for NCDIs, from 0.7%–12.9% for NCDs and 0.1%–5.7% for injuries. In Liberia, 74.7% of expenditures for NCDIs were out-of-pocket, exceeding the proportion of out-of-pocket expenditure for other disease areas, such as malaria (60%), TB (48%), HIV/AIDS (30%), and reproductive, maternal, neonatal, child, and adolescent health (19%).29 In Ethiopia, 68% of expenditures for NCDIs were out-of-pocket.26
Commissions’ Recommendations on Prioritization for NCDI Conditions and Health-Sector Interventions (Phase 1b)
As of July 2020, 7 commissions completed a prioritization exercise for NCDI disease conditions and health-sector interventions (Unpublished Haiti NCDO Poverty Commission report).26,29–33 The commission in Ethiopia conducted a prioritization exercise for an expanded set of NCDI health interventions but not for disease conditions. Prioritization exercises had also been initiated in Mozambique, Sierra Leone, Uganda, Zimbabwe, and Zambia, though they were not yet completed and subsequently not included here. After compiling and analyzing data on the burden, severity, disability, and equity metrics from GBD, and undergoing a commission review and validation, the 6 commissions that had completed the process and had prioritized among NCDI conditions selected between 14 and 48 conditions for prioritization (Table 3). Overall, 75 of 211 total NCDI conditions were selected by at least 1 commission. Fifteen conditions were selected by all 6 commissions. These conditions included asthma, breast cancer, cervical cancer, diabetes mellitus type 1, diabetes mellitus type 2, epilepsy, hypertensive heart disease, intracerebral hemorrhage, ischemic heart disease, ischemic stroke, major depressive disorder, motor vehicle road injuries, rheumatic heart disease, sickle cell disorders, and subarachnoid hemorrhage. An additional 12 conditions were selected by at least 4 of the 6 commissions.
Results of National NCDI Poverty Commissions Prioritization of NCDI Conditions and NCDI Health-Sector Interventions
Six commissions considered 65 health-sector NCDI-focused interventions recently recommended as a package for EUHC. Thirty-two interventions were selected by a majority (>/=4) of the commissions, including 18 that were selected by all commissions (Table 4). Among these 32 interventions, 19 targeted the health center level, 6 targeted first-level hospitals, 4 at referral/specialty hospitals, 2 for population-level mass media messages, and 1 at the community level. These interventions included 4 surgical “packages” at various levels of the health system and packages for palliative care and rehabilitation services. Of the 18 interventions selected by all commissions, 17 were recommended as “high-priority” EUHC interventions by DCP3. The commission in Ethiopia conducted the prioritization exercise considering all 235 health-sector interventions they had identified and selected 90 interventions as high-priority. Including the commission in Ethiopia, the annual cost across the 7 commissions of the prioritized interventions at the target intervention coverage assigned by each commission ranged from US$4.70–US$13.70 per capita. This amount of per capita expenditure ranged from 9.7% (Haiti) to 35.6% (Tanzania) of the most recently reported total health expenditure per capita and from 0.6% (Ethiopia) to 4.0% (Malawi) of gross domestic product per capita at the time of the respective analyses.
Most Commonly Selected Conditions and Corresponding Prioritized Health Sector Interventions by 6 Commissions Conducting Prioritization Exercises by Both Disease Conditions and Health Sector Interventions (Displaying Conditions and Interventions Selected by >/= 4 Commissions)
The annual cost across the 7 commissions of the prioritized interventions at the target intervention coverage assigned by each commission ranged from US$4.70–US$13.70 per capita.
RESULTS OF EVALUATION
Responses were received from each of the 9 commissions formally established in Round 1. Findings were categorized according to the 3 overall NCDI Poverty Commission objectives: “Understanding NCDIs of Poverty,” “Planning and Implementation of NCDI Interventions,” and “Governance and Coordination for NCDIs” (Figure 2). Respondents provided key contextual information on successes achieved and challenges experienced by the national commissions (key aspects highlighted in Supplement Tables 3 and 4). Most respondents reported that their respective commissions improved their understanding of NCDI epidemiology in relation to poverty (n=7). However, only a minority of respondents reported improvements in understanding of gaps in current NCDI service delivery (n=2) or household expenditures and impoverishment by NCDIs (n=2). All country respondents indicated that their respective commissions had informed the development of national NCDI plans or strategies, and most reported provision of valuable evidence for health system planning (n=7) and contribution to defining essential health service packages (n=6). Several respondents reported contributions by their respective commissions for health insurance benefits packages (n=3) and the design of innovative or integrated services platforms (n=2). There was a strong theme of commissions supporting the governance of coordination of NCDIs, with most respondents indicating that their commissions altered perceptions of NCDIs by key policy makers (n=8), catalyzed the formation of broader coalitions for NCDIs (n=6), and enhanced capacity of the Ministry of Health in their NCDI response (n=7).
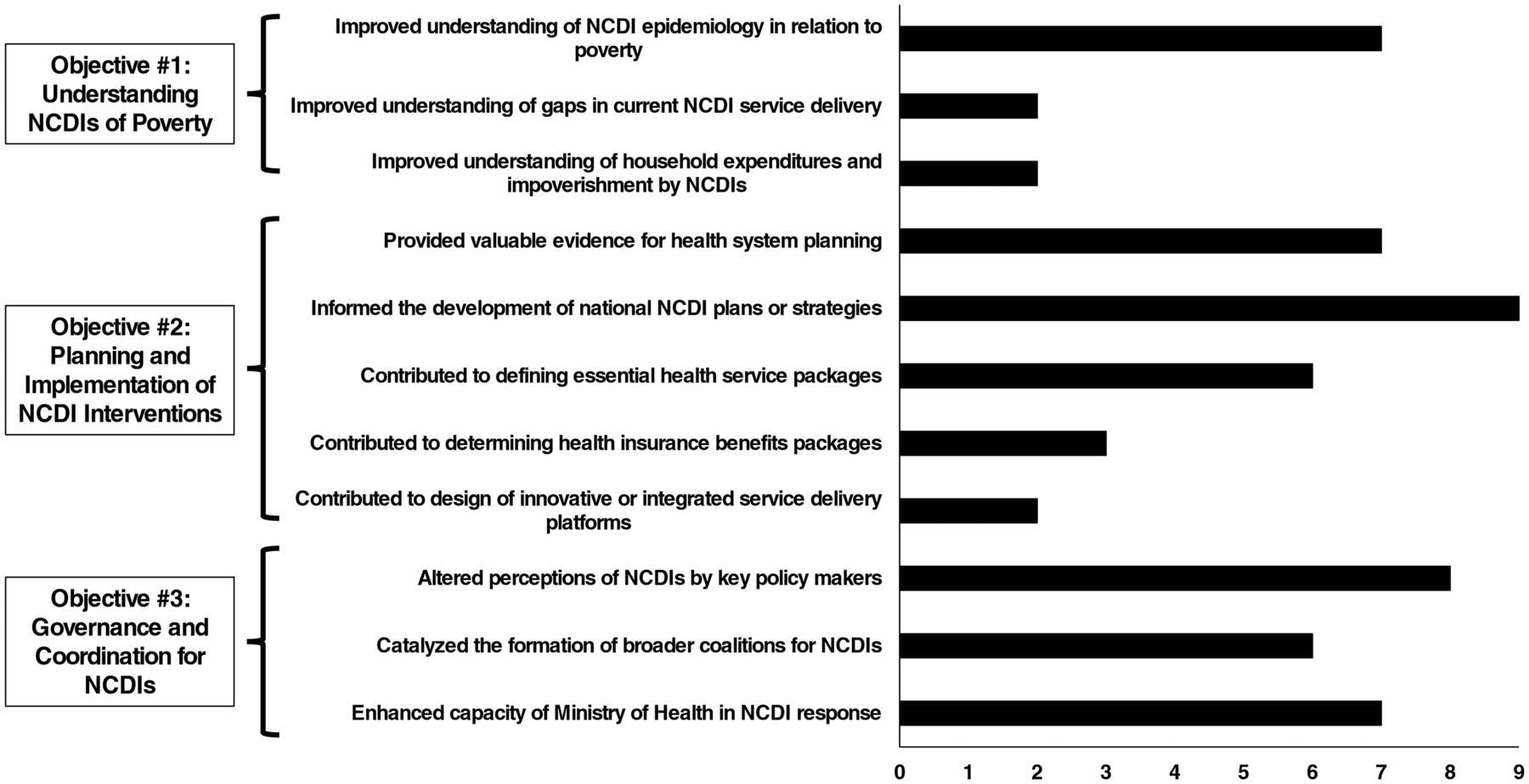
Frequency of National Noncommunicable Diseases and Injuries Poverty Commissions Reporting Key Outcomes in Evaluation Surveys and Qualitative Interviews, by Thematic Area (n=9)
Abbreviation: NCDI, noncommunicable diseases and injuries.
DISCUSSION AND NEXT STEPS
We have described the establishment, structure, and findings of national- and state-level NCDI Poverty Commissions established in 16 LLMICs with significant populations living in extreme poverty. The NCDI Poverty Commissions represent a coordinated effort to quantify the comprehensive burden of NCDIs and provide evidence-based recommendations on health-sector interventions to strengthen NCDI services under commitments to UHC.
The NCDI Poverty Commissions represent a coordinated effort to quantify the comprehensive burden of NCDIs and provide evidence-based recommendations on health-sector interventions to strengthen NCDI services under commitments to UHC.
Current expenditure on NCDIs reported by the commissions varied widely by country, though these findings may be subject to high variability and low reliability of national health accounts.34 The commissions estimated that to implement the prioritized health-sector NCDI interventions for a substantial target population would require an additional US$4.70–US$13.70 per capita, or approximately 9.7%–35.6% of current total health expenditure (or 0.6%–4.0% of current gross domestic product). The commissions in Malawi and Tanzania established more expansive criteria for selecting health-sector interventions to drive dialogue and advocacy for health system expansion and investment. Commissions in Nepal and Kenya opted for a more targeted approach to selecting interventions to focus advocacy on key interventions currently lacking in their respective health systems. The overall EUHC health benefits package was previously estimated to cost US$79 per person at 80% population coverage in low-income countries, representing an additional investment of 8.0% of the 2015 gross national income.27 Interventions to reduce mortality from NCDIs comprised at least 37.6% of these EUHC estimated costs, not including substantial costs of interventions targeting the reduction of disability from NCDIs. The interventions prioritized and costed by the commissions represent a more conservative incremental intervention coverage target (i.e., 30%) and focus on a smaller subset of NCDI interventions, though still include a wide range of medical, surgical, mental health, palliative care, and rehabilitation services, as well as indirect costs for laboratory services, infrastructure, administration, and management.
A recent analysis by the Lancet NCDI Poverty Commission showed that this level of additional expenditure for NCDIs may be possible within domestic financing under conditions of strong economic growth, increased tax revenues, and greater proportional allocation of government expenditures to health consistent with recent targets.5,35 However, such conditions may be unlikely in most LLMICs, particularly in the context of severe economic challenges incurred during the coronavirus disease (COVID-19) pandemic, and external development assistance will be required to finance this critical set of interventions.
Most commissions identified opportunities to integrate prioritized health-sector interventions into existing platforms to improve efficiencies and facilitate operationalization. Decentralization may rely on training and task optimization for nurses and other mid- to low-level cadres of the health workforce, and clustering of services based on intervention properties.36,37 Further efforts to more accurately define additional interventions within national contexts are needed to inform the development of essential health service packages, health insurance coverage schemes, and national financing priorities. Intersectoral policies were not explicitly prioritized and costed by the commissions and require further consideration given their vital role in the prevention of NCDIs.
The urgent need for strong integrated health systems to mitigate and address the adverse effects of NCDs in LLMICs has been magnified by the COVID-19 pandemic.
The urgent need for strong integrated health systems to mitigate and address the adverse effects of NCDs in LLMICs has been magnified by the COVID-19 pandemic.38,39 NCDI Poverty Commissions provide an opportunity for local definition and accountability for a context-specific and locally relevant NCDI agenda under rapidly evolving epidemiology and health system constraints. National commissioners highlighted the impact of these commissions in changing the traditional perceptions and framing of NCDIs with a focus on severe conditions affecting poor, rural populations at young ages. The priority-setting process utilized in this analytic framework was additive and contributory to national strategic and operational planning efforts and packages of essential services, core components to health system readiness, and achievement of commitments to UHC. The commissions provided a productive forum for policy makers to meet with academic and implementing stakeholders to critically analyze and consider available data and formulate evidence-based recommendations. National commissioners highlighted the role of commissions in strengthening in-country public-sector capacity in the response to NCDIs and expanding perceptions of NCDIs by key policymakers. Evaluation of a group of these commissions demonstrated substantial contributions of the commissions in informing national efforts in strategic and health system planning for NCDIs as well as the understanding and capacity of key governance structures for the NCDI response at a national level.
The collective experience of the commission processes and findings presented here has informed the establishment of the NCDI Poverty Network.40 The NCDI Poverty Network aims to catalyze technical and financing partnerships to improve the understanding, awareness, investment, and outcomes for individuals living with NCDIs in settings of extreme poverty. National commissions will further assess the current availability and organization of these interventions in both public and private-sector facilities, with a particular focus on integrating and optimizing human resource availability and capacities. In addition, national commissions will play a key role in defining, piloting, and scaling potential facility-based delivery models for severe conditions impacting younger populations, such as “PEN-Plus.”41 The NCDI Poverty Network will aim to promote cross-border collaboration for an expanded NCDI agenda, build programmatic and research capacity, and establish global financing partnerships to support the availability and coverage of NCDI interventions. These will be necessary steps to fulfill national commitments to UHC for populations facing the double burden of extreme poverty and disproportionately suffering from the physical and economic consequences of a highly diverse array of NCDIs.
Acknowledgments
We would like to acknowledge the dedication and commitment of all of the participating members, research assistants, and administrative staff that supported the National NCDI Poverty Commissions. We also thank Maia Olsen, Paul Park, Alma Adler, Catherine Player, Kelsey Soderberg, and Lauren Brown of the NCDI Poverty Secretariat for their dedicated support in the administration and implementation of this project. Other organizations that provided indirect or in-kind support of the National NCDI Poverty Commissions included Partners In Health, Department of Global Health and Social Medicine at Harvard Medical School, and the Harvard Medical School Center for Global Health Delivery-Dubai. We thank Miriam Schneidman and the World Bank for their in-kind support of the Knowledge Exchanges. The funding sources had no role in the design or content of the study design or analyses presented in this report. This manuscript is dedicated to the memory of our teacher and mentor Professor James Hakim, who died from complications of COVID-19 during the publication of this manuscript. Professor Hakim was a valiant leader and healthcare champion, and he will remain an inspiration to us all.
Authors in Noncommunicable Disease and Injuries Poverty National Commissions Authorship Group
Anand K Sahu, National Health Mission, Chhattisgarh, India;Roodney Dupuy, Le Ministère de la Santé Publique et de la Population, Port-au-Prince, Haiti; Erjesa Waqo, Kenya Ministry of Health, Nairobi, Kenya; Zoe Doe, Liberia Ministry of Health, Monrovia, Liberia; Jacquelin Pierre, Partners In Health, Monrovia, Liberia; Justin Haruna, PIVOT, Ranomafana, Madagascar; Abha Shrestha, Department of Community Medicine, Kathmandu University School of Medical Sciences, Dhulikhel, Nepal; Marta Lado, Partners In Health, Kono, Sierra Leone; Chembe Kachimanga, Partners In Health, Kono, Sierra Leone; James Hakim, College of Health Sciences, University of Zimbabwe, Harare, Zimbabwe.
NCDI Poverty Network Secretariat Authors
Chantelle Boudreaux, Program in Global NCDs and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA; Matthew M Coates, Division of Global Health Equity, Brigham & Women’s Hospital, Boston MA; Andrew Marx, Program in Global NCDs and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA; Amy McLaughlin, Partners In Health NCD Synergies, Boston, MA; Arielle W Eagan, Program in Global NCDs and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA; Alex Kintu, Program in Global NCDs and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA; Wubaye W Dagnaw, Partners In Health NCD Synergies, Boston, MA; Program in Global NCDs and Social Change, Department of Global Health and Social Medicine, Harvard Medical School, Boston, MA; Ethiopia Ministry of Health, Addis Ababa, Ethiopia.
Funding
The Leona M. and Harry B. Helmsley Charitable Trust provided major funding for this project. We acknowledge the funding support of the Norwegian Agency for Development Cooperation for the Ethiopia NCDI Commission and the Inter-American Development Bank for the Haiti NCDI Poverty Commission.
Author contributions
All authors contributed significantly to the design, implementation, measurement and reporting of the program described in this manuscript. Additionally, all authors contributed to the data collection, data interpretation, and writing of the main manuscript. All authors have reviewed the full manuscript and have provided written feedback.
Competing interests
None declared.
Footnotes
A complete list of the authors in the Noncommunicable Diseases and Injuries (NCDI) Poverty National Commissions Author Group and the NCDI Poverty Network Secretariat appears at the end of the article.
Notes
Peer Reviewed
First published online: August 3, 2021.
Cite this article as: Gupta N, Mocumbi A, Arwal SH, et al. Prioritizing health-sector interventions for noncommunicable diseases and injuries in low- and lower-middle income countries: national NCDI Poverty Commissions. Glob Health Sci Pract. 2021;9(3):626-639. https://doi.org/10.9745/GHSP-D-21-00035
- Received: February 21, 2021.
- Accepted: June 1, 2021.
- Published: September 30, 2021.
- © Gupta et al.
This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visit https://creativecommons.org/licenses/by/4.0/. When linking to this article, please use the following permanent link: https://doi.org/10.9745/GHSP-D-21-00035









{kind=link}
{kind=link}