


Figures & Tables
Figures
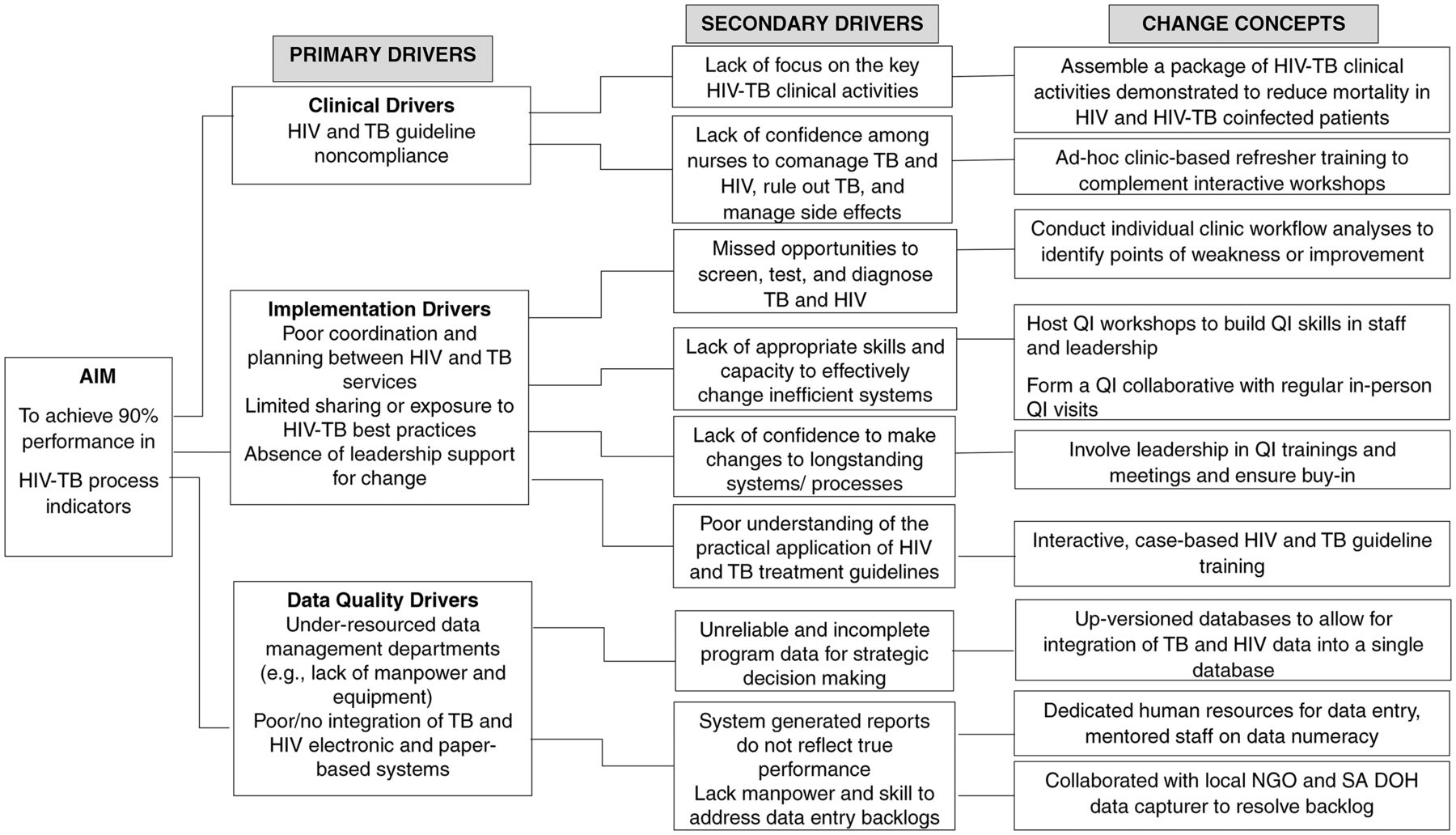
- FIGURE 1
Change Theory Based on Primary and Secondary Drivers of Poor Performance in Integrated HIV-TB Services and Change Concepts Used in a Quality Improvement Intervention for HIV/TB Service Integration in KwaZulu-Natal, South Africa
Abbreviations: NGO, nongovernmental organization; QI, quality improvement; SA DOH, South African Department of Health.
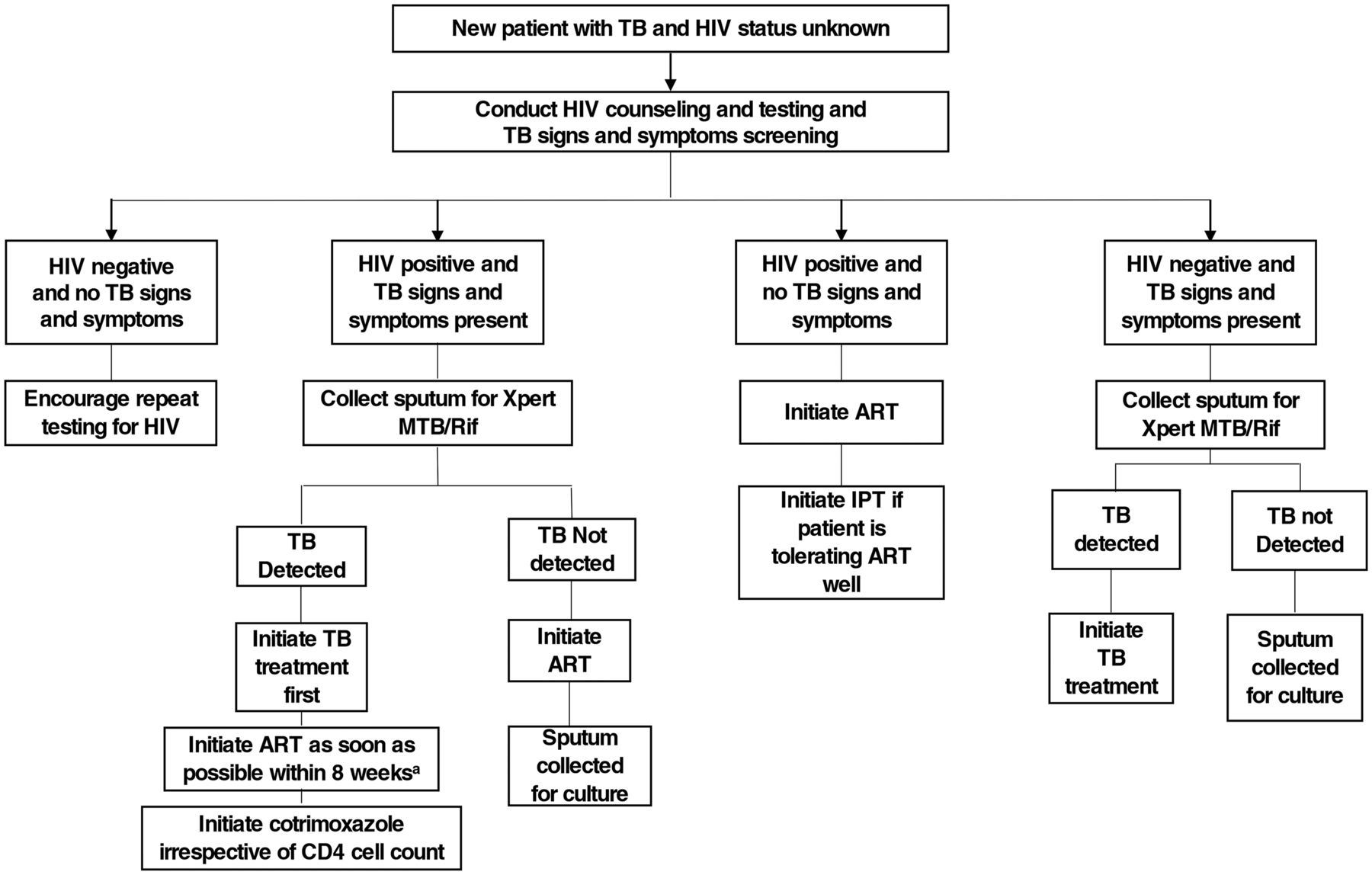
- FIGURE 2
Key HIV-TB Services Care Algorithm Training Tool Used in a Quality Improvement Intervention for HIV/TB Service Integration in KwaZulu-Natal, South Africa
Abbreviations: ART, antiretroviral therapy; IPT, isoniazid preventive therapy; Xpert/MTB/Rif, a rapid, molecular, cartridge-based test used for TB diagnostics that provides an immediate rifampicin resistance result.
a For HIV-TB coinfected patients: If CD4<50 cells/µl, initiate ART within 2 weeks of starting TB treatment AND if CD4>50 cells/µl, initiate ART within 2–8 weeks of starting TB treatment.
- FIGURE 3
xmr Charts of Monthly Performance in HIV-TB Process Indicators in a Quality Improvement Intervention for HIV/TB Service Integration in KwaZulu-Natal, South Africa (a) Percentage of Eligible New ART Patients Initiated on IPT; (b) Percentage of ART Patients With a Viral Load Test Conducted; (c) Percentage of PHC Clinic Attendees Screened for TB; (d) Percentage of HIV Target Achieved; (e) Percentage of HIV-TB Coinfected Patients Initiated on ART
Abbreviations: ART, antiretroviral therapy; IPT, isoniazid preventive therapy; PHC, primary health care.

Tables
- TABLE 1.
Definitions of HIV-TB Process Indicators Used in the Quality Improvement Intervention to Integrate HIV-TB Services in KwaZulu-Natal, South Africa
HIV-TB Process Indicator Abbreviation Definition HTS for PHC clinic attendees HTS Percentage of patients that accessed HIV tests, expressed as a percentage of the clinics’ HIV testing targeta
Numerator: Number of patients tested for HIV
Denominator: Clinic assigned target for HTSTB screening among PHC clinic attendees TB screening Percentage of clinic attendees screened for TB signs or symptomsb
Numerator: Number of clinic attendees screened for TB signs and symptoms (adults and children)
Denominator: Clinic headcount (Number of people accessing any health services at a facility during a specified period)Initiating IPT among eligible new ART patients IPT initiation Percentage of new ART patients initiated onto IPT
Numerator: Number of new ART patients initiated on IPT
Denominator: Number of new ART patients with no signs or symptoms of TBART initiation among TB/HIV coinfected patients ART initiation Percentage of TB/HIV coinfected patients initiated on ART
Numerator: Number of TB/HIV coinfected patients initiated on ART
Denominator: Number of confirmed TB patients tested positive for HIVVL testing at month 12 after ART initiationc VL testing Percentage of eligible ART patients who had a VL test at month 12 after ART initiation
Numerator: Number of ART patients who received a VL test at month 12 after ART initiation
Denominator: Number of ART patients eligible for a VL test at month 12 after ART initiationAbbreviations: ART, antiretroviral therapy; HTS, HIV testing services; IPT, isoniazid preventive therapy; PHC, primary health care; VL, viral load.
↵a All clinics receive a monthly target for HIV Testing Services from their respective District Offices.
↵b TB signs and symptom screening refers to the verbal screening checklist which documents the common signs and symptoms of TB (current cough of any duration, fever for >2 weeks, drenching night sweats, Unexplained weight loss of >1.5kg in a month).
↵c According to the South African National Department of Health National Consolidated guidelines, a viral load test is required at month 6 and month 12 after ART initiation and annually thereafter. This study focused on the month 12 viral load only.
- TABLE 2.
Summary of Changes in HIV-TB Process Indicators Used in the Quality Improvement Intervention to Integrate HIV-TB Services in KwaZulu-Natal, South Africa
HIV-TB Process Outcomes Proportions (95% CI) AbsoluteDifference P Value Clinicsa(N=20) PDSA CyclesMean, (Range) Baseline Post-QI Intervention HTS 84.8 (75.5,95.3) 94.5 (89.3,99.9) 9.7 .110 12 3 (1–7) TB screening 76.2 (65.4, 88.9) 85.2 (78.7,92.2) 9.0 .040b 17 4 (1–9) IPT initiation in new ART patients 15.9 (4.8,52.5) 76.4 (66.3,88.1) 60.5 .019b 20 4 (1–11) ART initiation in HIV-TB patients 95.8 (93.3,98.3) 94.1 (89.7,98.6) −1.7 .481 3 1 (1–3) Viral load monitoring 61.4 (56.4,66.8) 74.0 (65.5,83.6) 12.6 .045b 20 4 (1–7) - TABLE 3.
District and Clinic Staff Trained in Quality Improvement Methods for a Quality Improvement Intervention for HIV/TB Service Integration in KwaZulu-Natal, South Africa
Staff Category Pool of Health Care Workers AvailableN=259 Actual Number Trained in QI Learning Session 1N = 63 Learning Session 2N=61 Learning Session 3N = 45 n (%) n (%) n (%) District Management Team TB program manager 3 2 (3) 1 (2) 2 (4) HIV/AIDS/Sexually transmitted infection and TB manager 2 2 (3) 2 (3) 2 (4) Training coordinator 2 2 (3) 2 (3) 0 Nurse supervisors 8 5 (8) 4 (6) 3 (7) Subtotal 15 Clinic Staff Categories Operations managers 19 11 (17) 9 (15) 9 (20) Professional nurses 85 6 (10) 11(18) 8 (18) Enrolled nurses/ enrolled nurse assistants 61 8 (11) 6 (10) 1(2) Data capturers 36 17 (27) 18 (30) 19 (42) Lay counselors 43 10 (16) 8 (13) 1 (2) Subtotal 244 - TABLE 4
Health Systems Weaknesses Identified and Associated Change Ideas for a Quality Improvement Intervention for HIV/TB Service Integration in KwaZulu-Natal, South Africa
HIV-TB Process Health Systems’ Weaknesses Identified Change Concepts HTS Relying only on patient requests or referrals for HIV testing. Introduced strategies to enhance provider-initiated testing: Offered group pretest counseling in all patients’ waiting areas
Implemented a daily roster system of staff to conduct pre-test counseling
Nurse in charge or designee to check accountability log daily
Missed opportunities to offer HTS to all patients Acute patients were overlooked for HTS services (e.g., wound care patients)
Redesigned clinic patient flow Ensure that acute patients are directed to lay counselors after vitals assessmentsa are conducted
If above not possible, then staff caring for acute patients were (i) trained in HIV testing and counseling and (ii) provided with the appropriate HTS stationery
HTS data inaccuracies caused by: Not completing HTS registers in real-time
Misplacing HTS registers
Daily data quality control checks Daily quality control of HTS registers and frequent audits of patient files and electronic data to ensure HIV status is known for all patients
Overdependence on lay counselors HTS viewed as the work of lay counselors
Lack of counseling skills among nurses to relieve/stand-in for lay counselors
Increasing the accountability and responsibility for the HTS program On-site HTS refresher training was held which addressed: pre- and post-test counseling messages, conducting HIV rapid tests, and data recording
Awareness of clinic target set by the district health office was disseminated
TB screening among PHC clinic attendees Missed opportunities to offer TB screening to all clinic attendees Centralized TB screening Made TB screening mandatory at an identified strategic point visited by all patients, such as, vitals assessmenta station
Visual prompts and reminders to conduct TB screening included large and colorful TB posters, printed and easily accessible signs, and symptoms checklists
Made TB screening mandatory for acute patients
Inaccurate TB screening data Data quality control checks Daily data quality control checks conducted by nurse in charge or designee to check:
Completeness and accuracy of daily TB screening register
Number of symptomatic patients and number of sputum samples sent for Xpert/ MTB Rifb testing
Quality control of clinic headcountc data:
Exclude patient representatives or family members
Subtract TB confirmed patients from the clinic headcount
Mass TB screening campaigns conducted in communities must be distinguishable from screening conducted in the clinic
IPT initiation among new ART patients Ambiguity in IPT initiation guidelines Nurses lack clarity on timing of IPT initiation
Individual nurses use own discretion to start IPT
Clarify IPT initiation timing and arrive at mutually agreed upon timing for initiation Each clinic team arrived at a common time to start IPT (e.g., 7,14, or 30 days after starting ART)
Agreed upon timing was documented and standardized for entire clinic
Confusion about roles and responsibilities of clinic staff Enhancing accountability and responsibility for IPT program Roles and responsibilities were assigned to all staff categories and documented
No system for identifying patients eligible for IPT Strategies to identify patients returning at the agreed upon time for IPT The “box system” -eligible patients’ files placed in a decorated box for easy identification, OR
Tagged files of eligible patients with stickers or red ink OR
The “diary system” reminder note in clinic diary to initiate IPT at next visit and note attached to patient file
Poor recording of IPT initiation date in clinic chart notes Refresher training on clinic stationery to document IPT Nurses directed to document start date in designated fields and data capturers shown where to find the start date
Nurses lack confidence to rule out TB Host a training for nurses, lay counselors, and data capturers highlighting the importance and potential benefit of IPT for HIV-infected patients Link this training with the TB screening training (above) to boost confidence to rule out TB
ART initiation among HIV-TB coinfected patients Patient chart notes for TB and ART kept separately TB and ART files not integrated
No unique identifier for TB and ART file
Combining ART and TB files For HIV-TB coinfected patients, ART and TB chart notes were physically combined
The district health office agreed upon a common unique identifier to be used
The TB module on the electronic ART database was activated to accommodate TB and ART data
Poor coordination between NIMART and TB nurses regarding ART and TB treatment initiation Refresher training for nurses Clarified patient flow for ART initiation visits in TB/HIV coinfected patients
Improved chart notes for ART and TB treatment start dates
VL monitoring at month 12 after ART initiation No system to identify patients eligible for month 12 VL tests Generate report from electronic system of patients due for VL Address the data capturing backlog of VL results and ART initiation
Draw on the assistance of local nongovernmental organizations and support partners for assistance with data capture
Generate VL reports from the data system to determine which patients have not had or are due for VL test (filter out deceased and transferred-out patients)
Tag/mark the files of patients due for VL for easy identification
Trace patients who were missed for a VL test
Abbreviations: ART, antiretroviral therapy; HTS, HIV testing services; IPT, isoniazid preventive therapy; NIMART, Nurse Initiated Management of Antiretroviral Therapy; PHC, primary health care; VL, viral load.
↵a Vitals assessments refers to general measures of well-being which typically include weight, body temperature, blood pressure measurements.
↵b Xpert/MTB RIF a rapid, molecular, cartridge-based test used for TB diagnostics that provides an immediate rifampicin resistance result.
↵c Clinic headcount refers to the total number of patients who accessed the clinic for any type of clinical service.
Supplemental material
- Supplement -
Supplement
- Supplement -
In this issue









{kind=link}
{kind=link}
{kind=link}
Statistics from Altmetric.com
Jump to section
Related Articles
Cited By...
- No citing articles found.