


The 2019–2020 Ebola virus disease (EVD) outbreak in the Democratic Republic of the Congo (DRC) was a tragic and significant threat to thousands of people in the DRC and West Africa in general. As of March 25, 2020, an estimated 3,462 people in the DRC have been infected and an estimated 2,267 people have died from this terrible virus. Since EVD was first characterized in 1976, there have been 38 country-specific outbreaks, including the outbreak in the DRC. The total estimated EVD deaths from 1976 to 2020 is 15,266. The median number of deaths for all 38 outbreaks is 29 with a range of 0 to 4,809 (Table 1).1,2
Country-Specific Ebola Virus Disease Outbreak Timeline
The EVD case fatality rate (CFR) can be 0 or reach 100%, depending on the scope and location of the outbreak (e.g., 2011 Uganda [1 case 1 death], Senegal 2014 [1 case, 0 deaths]). Although there are 4 different types of Ebola virus,3 generally speaking, the EVD CFR averages about 50%.4 The 2015 outbreak in Guinea, Liberia, and Sierra Leone infected an estimated 28,610 people and killed 11,308 with a CFR of approximately 40%. Without question, EVD is an important and daunting public health issue for Africa and potentially for the world.
However, EVD is an epizootic infection with periodic human exposure and transmission. Since its emergence in 1976; the virus remains an uncomfortable human pathogen. It kills too fast, kills too many, and is not easily transmitted; thus, human outbreaks are limited, and its pandemic potential is moderate to low. It has not yet achieved equilibrium with its human host as it apparently has with its bat host. Furthermore, EVD’s 40%–50% CFR in humans may be considered evolutionarily unsound in many respects for a successful human pathogen.
But, the real issue concerning EVD is disease sensationalism. This can be characterized as an unfounded perception of a global emergency, not necessarily anchored in the epidemiology, pandemic potential, and total mortality of a pathogen. Rather, it appears the classification of a global emergency is based more on the political ramifications, the newsworthiness of the disease de jour, and yes, financial aspects and funding streams of a declared emergency for an emerging and/or reemerging infection. Tragically, more than 11,000 died of EVD in Guinea, Liberia, and Sierra Leone. However, it should be recognized that far more individuals (especially children under 5 years old) died since 1976 in these countries from preventable and treatable but less exotic infections. Should there not be a “moral claim” by the world’s children on emergency resources as well?
In 2014, the Obama administration submitted an emergency funding request, and in 2015, Congress authorized an appropriation of approximately US$5.4 billion in an omnibus emergency bill to combat EVD spread, protect America from an EVD outbreak, and support the development of an EVD vaccine.5 Notably, this appropriation exceeded the total 2015 authorization of US$3.13 billion for all U.S. government assistance for maternal, child, reproductive health, malaria, nutrition, and neglected tropical diseases by US$227 million.6 Did EVD epidemiology and national/global risk justify the emergency bill investment? Perhaps, perhaps not.
Clearly emerging and reemerging infections are important and need to be handled with interventions that mitigate spread and minimize mortality, coupled with adequate and sustained epidemic preparedness. Indeed, there have been concrete benefits for managing future internationally-important outbreaks such as better infection prevention techniques and equipment, improved surveillance methods, better international response, and a better understanding of behavioral determinants and the basic biology of such viruses and techniques for vaccine and therapeutic development. Furthermore, in some countries, lessons learned from the severe acute respiratory syndrome and Middle East respiratory syndrome outbreaks are being applied to the present COVID-19 pandemic.
Hyperinflated, news-based fear; questionable statistical models; and global emergency statements should not justify disproportionate allocations of time and effort on a specific issue of lesser epidemiological impact when millions of people are at risk from diseases that can be prevented, treated, and cured.
It is a sad and tragic fact that from 1976 to present, approximately 34,600 individuals have been infected with EVD and approximately 15,200 have died from EVD (CFR=44.1%) (Table 1). It is noteworthy that the U.S. Centers for Disease Control and Prevention predicted that the 2014–2016 West African EVD outbreak could have infected more than 1.4 million people in Liberia and Sierra Leone alone7:
Extrapolating trends to January 20, 2015, without additional interventions or changes in community behavior (e.g., notable reductions in unsafe burial practices), the model also estimates that Liberia and Sierra Leone will have approximately 550,000 Ebola cases (1.4 million when corrected for underreporting).
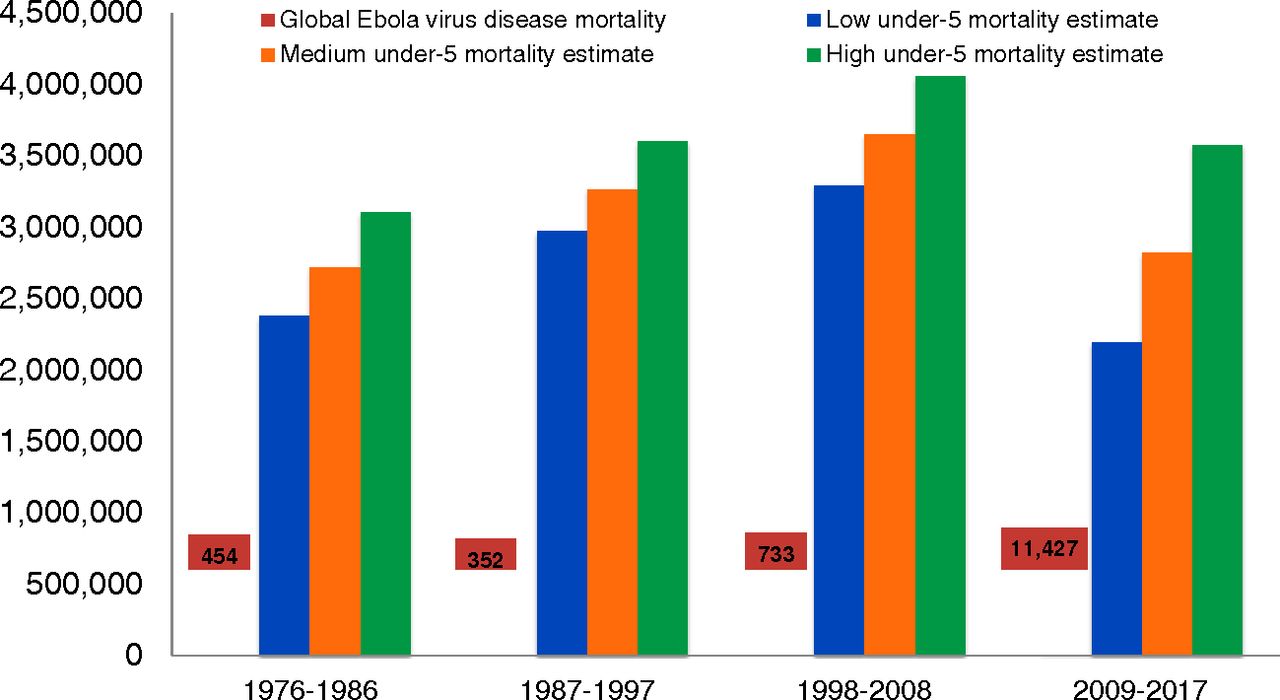
Over the period from 1976 to 2017, in the DRC alone approximately 12.43 million children under 5 years old have died, mostly from preventable and curable childhood diseases (Table 2)8 (Figure).2 This number dwarfs the 15,266 people who have died from EVD globally over the same period. Furthermore, at the global level, annually, an estimated 5.3 million children under 5 years old die from preventable and curable causes worldwide.9 Which qualifies as a more urgent and important global health emergency: global EVD or global under-5 mortality?
Under-5 Deaths in the Democratic Republic of the Congo from 1976–20178a
The term public health emergency of international concern (PHEIC) is defined in the International Health Regulations (2005) as:
An extraordinary event, which is determined, as provided in these Regulations: to constitute a public health risk to other States through the international spread of disease; and to potentially require a coordinated international response. This definition implies a situation that: is serious, unusual or unexpected; carries implications for public health beyond the affected State’s national border; and may require immediate international action.10
The PHEIC definition accurately describes an epidemiological emergency. However, it falls short on quantifying the impact of the emergency on existing and/or potential morbidity and mortality on a national, regional, or global scale. As noted, the burden of disease for children under 5 years old dramatically exceeds the cumulative global morbidity and mortality from EVD. Considering measles alone, from January 2019 through November 2019, the United Nations Children’s Fund reported 5,000 measles deaths (90% in children under 5 years old) in the DRC, with over 200,000 measles cases.11,12 Globally, measles surged in 2019 and killed about 140,000 worldwide,13 which is about 9.2 times the total number of deaths caused by EVD in its 43-year history as a human pathogen.
Clearly, great success has been achieved over the last 25 years in reducing deaths in children under 5 years old. However, in my view, the “unfinished agenda for child survival,”14 also qualifies as a public health emergency that should be of international concern. It deserves heightened attention by the governments, multilateral and bilateral donors alike, and should not be marginalized. Every day, approximately 14,500 children under 5 years old die, the equivalent of 35 Boeing 747 plane crashes.15 Clearly, global child mortality fits the World Health Organization’s definition of a “Grade 3” emergency and should be categorized as such.16 We need increased and continuous global investment in child survival and sustainable health system development.17 The moral claim of the world’s children should no longer be ignored.
The “unfinished agenda for child survival,” also qualifies as a public health emergency that should be of international concern.
Notes
First published online: May 19, 2020
Cite this article as: Barbiero VK. Ebola: a hyperinflated emergency. Glob Health Sci Pract. 2020;8(2):178-182. https://doi.org/10.9745/GHSP-D-19-00422
- Received: December 26, 2019.
- Accepted: April 7, 2020.
- Published: June 30, 2020.
- © Barbiero.
This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visit http://creativecommons.org/licenses/by/4.0/. When linking to this article, please use the following permanent link: https://doi.org/10.9745/GHSP-D-19-00422









{kind=link}