


Figures & Tables
Figures
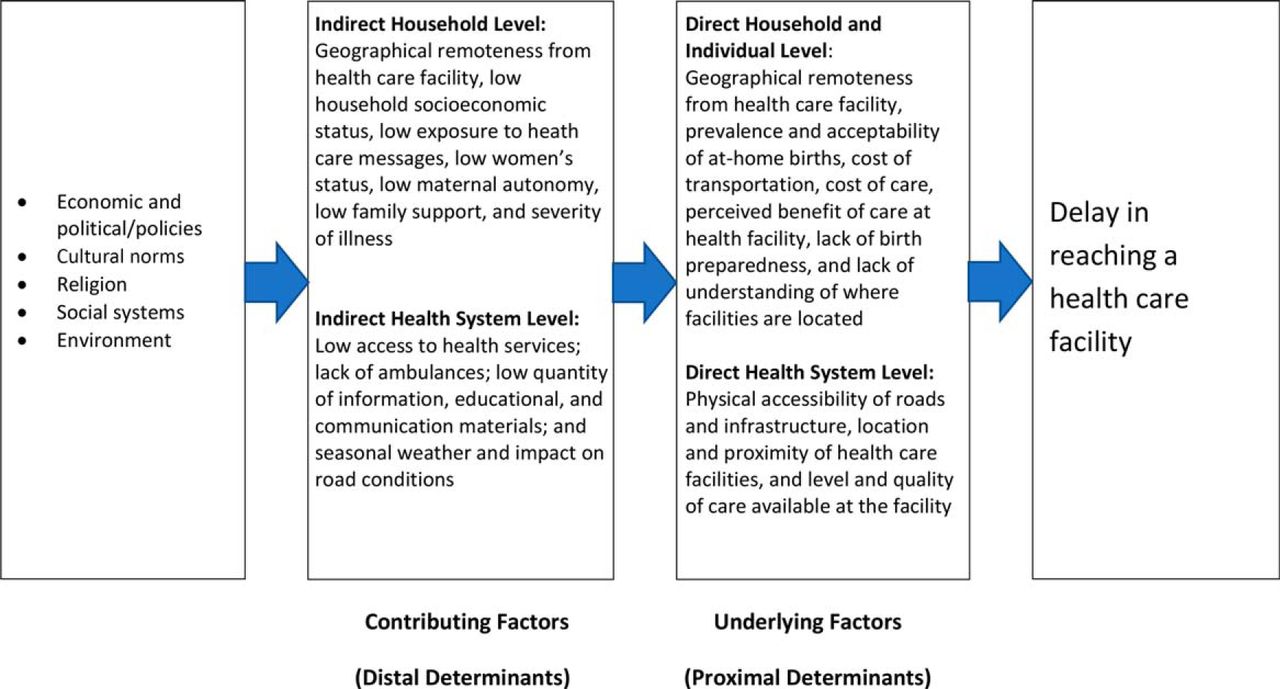
- FIGURE 1
Second Delay: Timely Access to Health Care
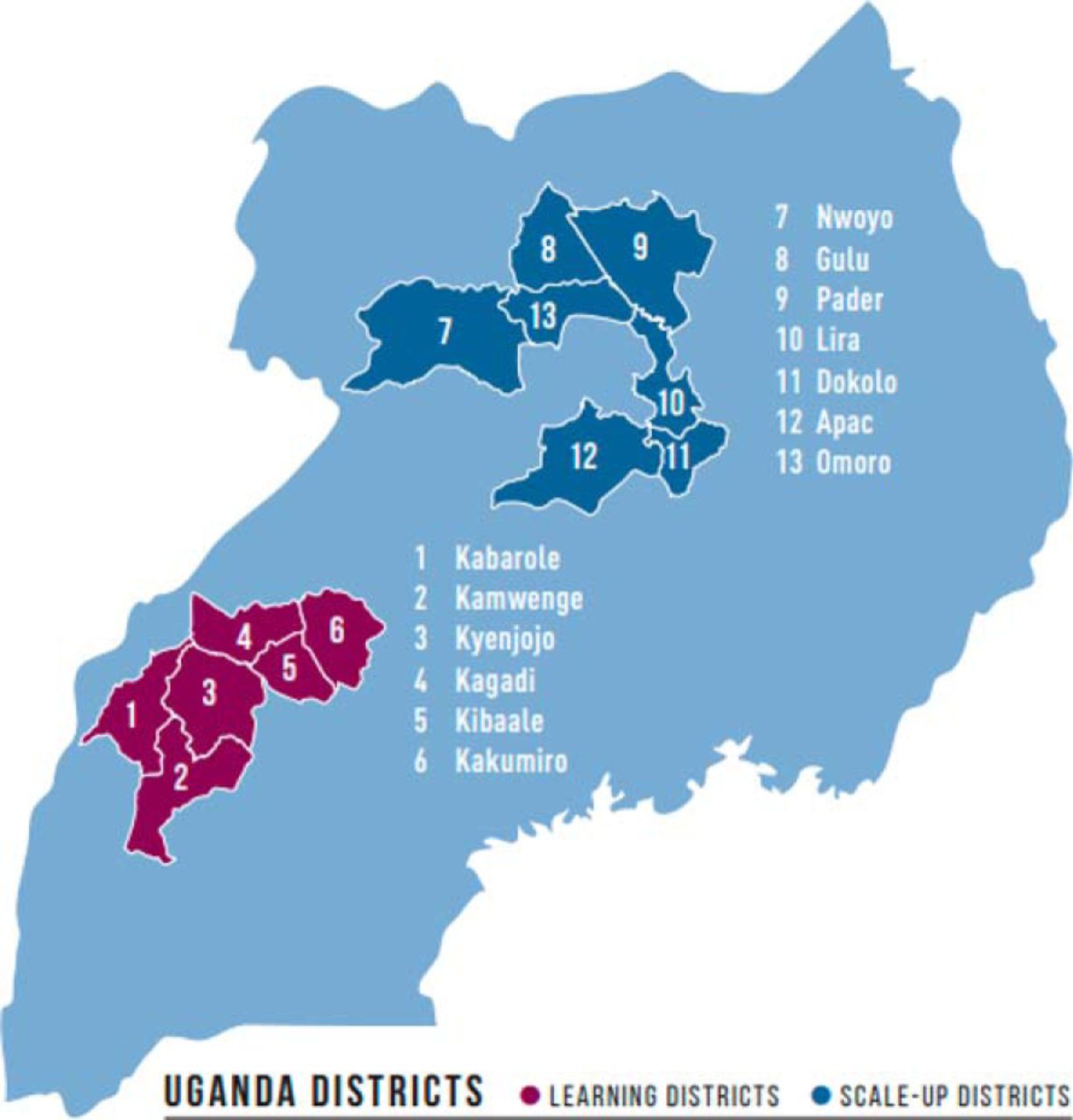
- FIGURE 2
SMGL Learning and Scale-Up Districts in Uganda
Source: Adapted from Saving Mothers, Giving Life. Results of a Five-Year Partnership to Reduce Maternal and Newborn Mortality: Final Report 2018. http://www.savingmothersgivinglife.org/docs/smgl-final-report.pdf. Accessed December 18, 2018.
- FIGURE 3
SMGL Learning and Scale-Up Districts in Zambia
Source: Adapted from Saving Mothers, Giving Life. Results of a Five-Year Partnership to Reduce Maternal and Newborn Mortality: Final Report 2018. http://www.savingmothersgivinglife.org/docs/smgl-final-report.pdf. Accessed December 18, 2018.

Tables
- TABLE 1.
Saving Mothers, Giving Life Strategies and Interventions to Reduce the Second Delay, 2011–2016
SMGL Strategies and Approaches Country-Specific Interventions Uganda Zambia Strategy 1. Decrease distance to skilled birth attendance by increasing the number of EmONC facilities Establish additional EmONC facilities and strengthen existing facilities to provide the following services 24 hours per day, 7 days a week, for all pregnant women in the district: Clean and safe basic delivery services
Quality HIV testing
Counseling and treatment (for woman, partner, and baby as appropriate)
Essential newborn care
24-hour availability of staff capable of managing delivery complications
When needed, timely facilitated referral to higher-level facility
Upgraded infrastructure to a sufficient number of public and private facilities in appropriate geographic locations and provided necessary equipment and commodities for EmONC service delivery
Hired midwives, medical officers, and anesthetists
Trained medical officers, anesthetists, midwives, and nurses in EmONC
Provided on-site mentorship of health facility teams using protocols
Upgraded infrastructure and provided necessary equipment to provide services for pregnant women in public and private facilities in appropriate geographic locations
Hired a sufficient number of skilled birth attendants and midwives
Trained doctors, midwives, and anesthetists in EmONC and the Electronic Logistic Management Information System
Provided on-site mentorship of health facility staff using protocols, forms, and drills
Strategy 2. Improve accessibility of EmONC facilities Create a communication and transportation referral system that operates 24 hours per day, 7 day per week, and: Is consultative, protocol-driven, quality-assured, and integrated (public and private)
Ensures that women with complications reach emergency services within 2 hours
Includes buying ambulances, motorcycles, motorbikes, and communication equipment like 2-way radios
Provides or renovates, where appropriate, temporary lodging in maternity waiting homes for women with high-risk pregnancies or who live more than 2 hours travel time to an EmONC facility
Provides service delivery vouchers and vouchers for transport to basic delivery care facilities and referral to higher-level facilities
Forms district-level transport committees to improve referral
Created district transportation committees to improve coordination of ambulances for referrals
Provided service and transportation vouchers to women for transportation to facilities nearest to them and access to antenatal care, delivery, and postnatal care services at the facilities
Trained village health teams to encourage birth preparedness and escort women to the facility
Procured ambulances to facilitate transportation for referral
Renovated maternity waiting homes
Repaired and procured 2-way radios where needed
Procured ambulances and motorcycle ambulances; strengthened district transportation committees; and ensured strategic placement of ambulances
Renovated and constructed maternity waiting homes
Strengthened district transportation committees to improve coordination of ambulance services
Trained Safe Motherhood Action Groups to encourage birth preparedness and escort women to the facility
Established village-level savings programs for pregnant women to encourage better planning for delivery
Abbreviations: EmONC, emergency obstetric and newborn care; SMGL, Saving Mothers, Giving Life.
- TABLE 2.
Changes in Outputs and Outcomes Related to Activities Conducted Under SMGL Strategies Addressing the Second Delay in SMGL-Supported Districts, Uganda
Baseline
June 2012
(105 facilities)Endline
Dec 2016
(105 facilities)% Relative changea Significance levelb Service delivery outcomesc Deliveries in all facilities 45.5% 66.8% +47% P<.01 Deliveries in EmONC facilities 28.2% 41.0% +45% P<.01 Deliveries in non-EmONC facilities 17.3% 25.8% +49% P<.01 Strategy 1: Decrease distance to skilled birth attendance by increasing the number of EmONC facilitiesd Facilities offering services 24 hours a day, 7 days a week 80.0% 87.6% +10% NS Facilities with electricity 57.1% 96.2% +69% P<.01 Facilities with running water 76.2% 100.0% +31% P<.01 Number of BEmONC facilities 3 9 +200% NA Number of CEmONC facilities 7 17 +143% NA Number of pregnant women who received antiretroviral therapy for the prevention of mother-to-child-transmission of HIV/AIDS 1,262 6,837 +442% NA Number of HIV-exposed infants receiving HIV prophylaxis 1,117 3,245 +191% NA Health facilities reporting that at least 1 doctor, nurse, or midwife is on staff 100.0% 100.0% 0% NS Strategy 2: Improve the accessibility of EmONC facilitiesd Institutional deliveries supported by Baylor transportation voucherse 0.9% 23.8% +258% P<.01 Health facilities that reported having available transportation (motor vehicle or motorcycle) 61.0% 59.0% −3% NS Health facilities that reported having communication equipment (including 2-way radio, landline, or cell phone with service) 93.3% 99.0% +6% P<.05 Abbreviations: BEmONC, basic emergency obstetric and newborn care; CEmONC, comprehensive emergency obstetric and newborn care; EmONC, emergency obstetric and newborn care; NA, not applicable; NS, not significant; SMGL, Saving Mothers, Giving Life.
↵a Percentage of change calculations are based on unrounded numbers.
↵b To test for significance, z scores based on the normal approximation to the binomial distribution were used to calculate P values.
↵c The number of facility deliveries was collected through the Pregnancy Outcome Monitoring data collection. The number of live births was estimated by applying crude birth rates (derived from the age-specific fertility rates among women of reproductive age enumerated in 2013 in the SMGL Uganda districts) to the baseline and endline district populations.
↵d The number of health facilities performing deliveries varied over the 5-year initiative. Health facility assessments results for Uganda were compiled from only the 105 facilities that maintained delivery capacity from baseline to endline.
↵e Transportation vouchers were introduced in April 2012 in the 3 Baylor districts; the system was rapidly scaled up with SMGL support.
- TABLE 3.
Changes in Outputs and Outcomes Related to Activities Conducted Under SMGL Strategies Addressing the Second Delay in SMGL-Supported Districts, Zambia
Baseline
June 2012
(110 facilities)Endline
Dec 2016
(110 facilities)% Relative changea Significance levelb Service delivery outcomesc Deliveries in all facilities 62.6% 90.2% +44% P<.01 Deliveries in EmONC facilities 26.0% 29.1% +12% P<.01 Deliveries in non-EmONC facilities 36.7% 61.1% +67% P<.01 Strategy 1: Decrease distance to skilled birth attendance by increasing the number of EmONC facilitiesd Facilities offering services 24 hours a day, 7 days a week 68.2% 96.4% +41% P<.01 Facilities with electricity 55.5% 92.7% +67% P<.01 Facilities with running water 90.0% 97.3% +8% P<.05 Number of BEmONC facilities 3 8 +167% NA Number of CEmONC facilities 4 5 +25% NA Number of pregnant women who received antiretroviral therapy for the prevention of mother-to-child transmission of HIV/AIDS 930 1,036 +11% NA Number of HIV-exposed infant receiving HIV prophylaxis 523 1,030 +97% NA Number of health providers hired — 89 — NA Health facilities reporting that at least 1 doctor, nurse, or midwife is on staff 90.0% 98.8% +10% P<.05 Strategy 2: Improve the accessibility of EmONC facilitiesd Health facilities that reported having available transportation (motor vehicle or motorcycle) 55.5% 72.7% +31% P<.01 Health facilities that reported having communications equipment (including 2-way radio, landline, or cell phone with service) 44.6% 100.0% +124% NA Health facilities that reported having an associated maternity waiting home 28.8% 48.8% +69% P<.01 Health facilities that reported having an associated Safe Motherhood Action Group 63.8% 96.3% +51% P<.01 Abbreviations: BEmONC, basic emergency obstetric and newborn care; CEmONC, comprehensive emergency obstetric and newborn care; EmONC, emergency obstetric and newborn care; NA, not applicable; NS, not significant; SMGL, Saving Mothers, Giving Life.
↵a Percentage of change calculations are based on unrounded numbers.
↵b To test for significance, z scores based on the normal approximation to the binomial distribution were used to calculate P values.
↵c The number of facility deliveries was collected through the Pregnancy Outcome Monitoring data collection. The number of live births was estimated by applying crude birth rates (derived from 2010 national census in Zambia) to the baseline and endline district populations.
↵d The number of health facilities performing deliveries varied over the 5-year initiative. Health facility assessments results for Zambia were compiled from only the 110 facilities that maintained delivery capacity from baseline to endline.
In this issue









{kind=link}
{kind=link}
{kind=link}
Statistics from Altmetric.com
Jump to section
Related Articles
Cited By...
- Strengthening Kampalas Urban Referral System for Maternal and Newborn Care Through Establishment of an Emergency Call and Dispatch Center
- Understanding maternity waiting home uptake and scale-up within low-income and middle-income countries: a programme theory from a realist review and synthesis
- What the percentage of births in facilities does not measure: readiness for emergency obstetric care and referral in Senegal
- Saving Mothers, Giving Life: It Takes a System to Save a Mother (Republication)
- Sustainability and Scale of the Saving Mothers, Giving Life Approach in Uganda and Zambia
- Saving Mothers, Giving Life: It Takes a System to Save a Mother
- Did Saving Mothers, Giving Life Expand Timely Access to Lifesaving Care in Uganda? A Spatial District-Level Analysis of Travel Time to Emergency Obstetric and Newborn Care
- Saving Mothers, Giving Life: A Systems Approach to Reducing Maternal and Perinatal Deaths in Uganda and Zambia
- Impact of the Saving Mothers, Giving Life Approach on Decreasing Maternal and Perinatal Deaths in Uganda and Zambia