


Figures & Tables
Figures
TBAs from Lufwanyama District, Zambia, attend a LUNESP training workshop to improve neonatal survival.
- Figure.
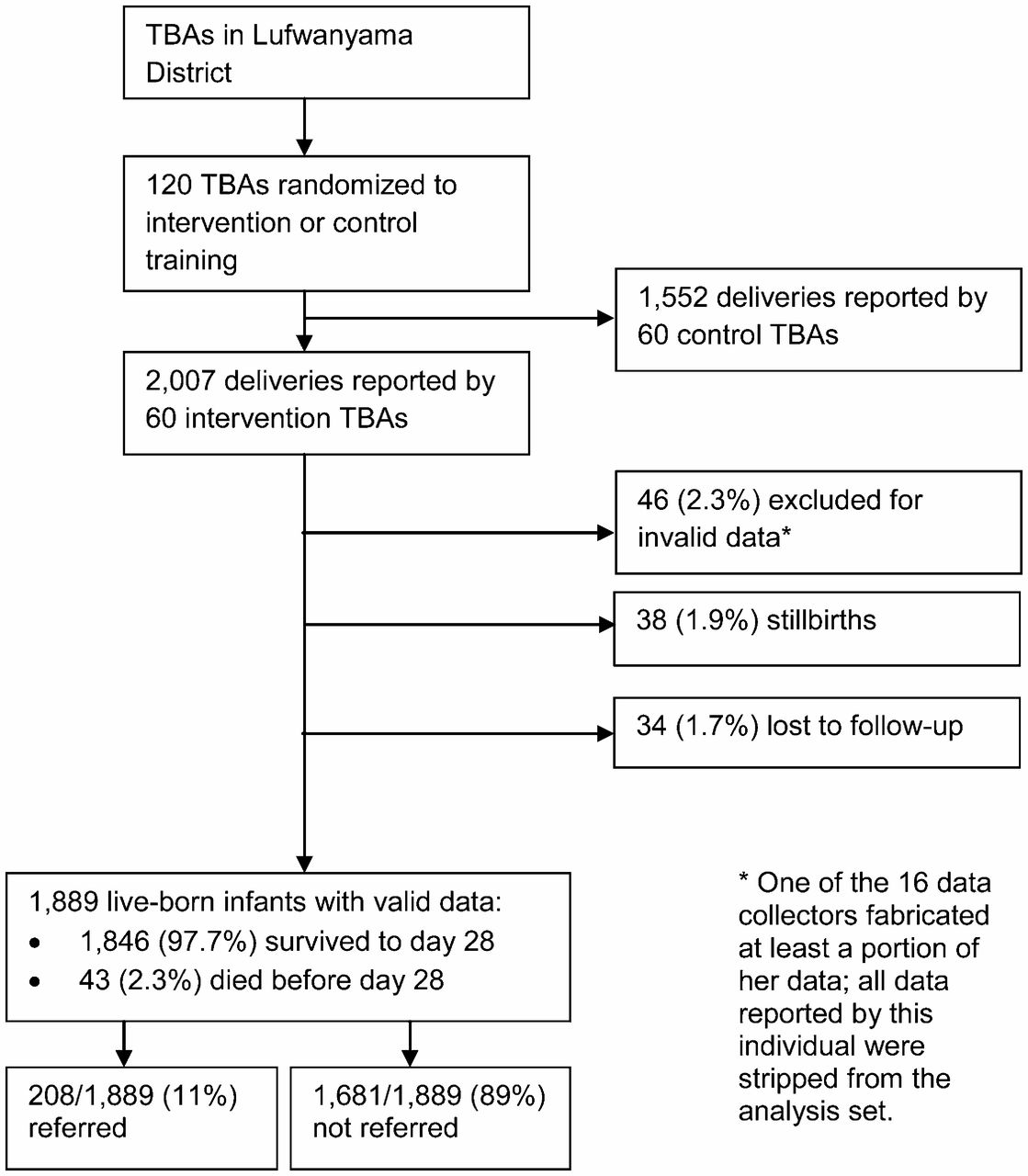
Data on Live-Born Neonates, June 2006–November 2008


Tables
- Table 1. Baseline Maternal and Infant Characteristics Stratified by Infant Vital Status at Day 28 of Life
Characteristic Infant Survivors (n = 1,846) Infant Deaths (n = 43) All Neonates (N = 1,889) P Value Maternal Characteristics Age, y, mean (SD) 25.3 (0.15) 25.7 (1.27) 25.3 (0.15) .77 Education (highest level attained), % .41 None 16.7 20.9 16.8 Some primary 69.2 58.1 68.9 Some secondary 13.8 20.9 14.0 Some higher 0.3 0.0 0.3 Marital status, % .84 Married 89.4 86.0 89.3 Widowed 0.8 0.0 0.8 Separated/divorced 2.5 4.7 2.5 Never married 7.3 9.3 7.4 No. of ANC visits attended, mean (SD) 3.3 (0.03) 3.2 (0.21) 3.3 (0.03) .67 Receipt of treatment IPT of malaria with SP, % 89.8 83.7 89.6 .20 Deworming treatments, % 65.9 55.8 65.6 .01 Folic acid supplementation, % 85.5 95.3 85.8 .07 Iron supplementation, % 92.5 90.7 92.5 .65 Tetanus toxoid, % 72.8 65.1 72.6 .26 Infant Characteristics Female, % 50.5 32.6 50.1 .02 Gestational age at birth, weeks, mean (SD) 38.0 (0.31) 43.0 (2.19) 38.1 (0.31) .33 Exclusively breastfed, % 96.8 86.0 96.6 <.001 Abbreviations: ANC, antenatal care; IPT, intermittent preventive therapy; SD, standard deviation; SP, sulfadoxine-pyrimethamine.
Characteristic Female, % 100 Age, y, mean (SD) 49.2 (0.79) Years working as TBA, mean (SD) 6.3 (0.81) Education Total years of education, mean (SD) 6.3 (0.48) Never attended school, % 5.0 Primary education only, % 78.3 Main occupation, % TBA 1.7 Farmer 98.3 Source(s) of training prior to LUNESP,a % Trained by family 11.5 Trained by community, not family 42.6 Trained by Lufwanyama DHMT 60.3 Trained by another government organization 33.3 Trained by an NGO 32.7 Abbreviations: DHMT, district health management team; LUNESP, Lufwanyama Neonatal Survival Project; NGO, nongovernmental organization; SD, standard deviation; TBA, traditional birth attendant.
↵a TBAs often received training from more than 1 source.
- Table 3. Sensitivity, Specificity, and Likelihood Ratios of Specified Reasons for Referral at Predicting a Fatal Outcome for the Referred Infant
Reason for Referrala Times Cited Prevalence % (95% CI) Sensitivity % (95% CI) Specificity % (95% CI) LR+ LR- Fever or felt hot 82 41.2 (34.3–48.4) 15.0 (3.2–37.9) 55.9 (48.3–63.3) 0.3 1.5 Had cough 80 40.4 (33.5–47.6) 25.0 (8.7–49.1) 57.9 (50.3–65.2) 0.6 1.3 Diarrhea 15 7.6 (4.3–12.2) 0.0 (0.0–16.1) 91.6 (86.5–95.2) 0.0 1.1 Refusing to feed 24 12.1 (7.9–17.4) 45.0 (23.1–68.5) 91.6 (86.6–95.2) 5.4 0.6 Sleepy or difficult to arouse 8 4.0 (1.8–7.8) 20.0 (5.7–43.7) 97.8 (94.3–99.4) 9.1 0.8 Floppy or poor muscle tone 18 9.1 (5.5–14.0) 25.0 (8.7–49.1) 92.7 (87.8–96.1) 3.4 0.8 Not making urine 22 31.9 (21.2–44.2) 57.1 (18.4–90.1) 71.0 (58.1–81.8) 2.0 0.6 Convulsions, fits, or seizures 8 4.1 (1.8–7.8) 15.0 (3.2–37.9) 97.2 (93.5–99.1) 5.4 0.9 Difficulty breathing 52 26.4 (20.4–33.1) 65.0 (40.8–84.6) 78 (71.1–83.8) 3.0 0.4 Rapid breathing 5 2.5 (0.8–5.8) 10.0 (1.2–31.7) 98.3 (95.1–99.6) 5.9 0.9 Chest wall in-drawing 1 0.5 (0.0–2.8) 0.0 (0.0–16.1) 99.4 (96.9–100.0) 0.0 1.0 Skin pustules or red rash 6 3.0 (1.1–6.5) 0.0 (0.0–39.0) 96.6 (92.8–98.7) 0.0 1.0 Infected umbilicus 3 1.5 (0.3–4.4) 5.0 (0.1–24.9) 98.9 (96–99.9) 4.5 1.0 Bulging fontanel 5 2.5 (0.8–5.8) 10.0 (1.2–31.7) 98.3 (95.1–99.6) 5.9 0.9 TBA thought baby appeared ill 164 82.8 (76.8–87.8) 95.0 (75.1–99.9) 18.5 (13.1–25.0) 1.2 0.3 Mother thought baby appeared ill 160 80.8 (74.6–86.0) 80.0 (56.3–94.3) 19.1 (13.6–25.7) 1.0 1.0 Otherb 62 NA NA NA NA NA No reason cited 8 NA NA NA NA NA Abbreviations: CI, confidence interval; LR+ and LR−, positive and negative likelihood ratios (clinically relevant LR+ and LR− values are in bold); NA, not applicable.
↵a TBAs were free to specify more than 1 reason for a given referral, so the total number of reasons for referral exceeds the number of neonates who were referred (208).
↵b Among the “other” reasons cited, those cited more than once included 12 citations for abdominal complaints (not making stool, swollen or tender belly, or diarrhea); 8 citations for inconsolable crying; 6 because the baby had been resuscitated at birth (all of which occurred during the first follow-up visit during week 1); 6 for skin rashes or sores; 4 for congenital defects or prematurity; 3 for respiratory complaints; and 3 for eye infections or discharge.
- Table 4. Survival of Neonates Stratified by the Subjective Severity of Illness Rating Assigned by the Referring TBA (N = 185)a
Outcome Severity Rating, n/N (%) Not sick Moderately sick Extremely sick Died 3/49 (6.1%) 6/113 (5.3%) 11/23 (47.8%) Survived 46/49 (93.9%) 107/113 (94.7%) 12/23 (52.2%) Total 49/185 (26.5%) 113/185 (61.1%) 23/185 (12.4%)b Abbreviation: TBA, traditional birth attendant.
↵a A total of 208 neonates were referred; TBAs provided a severity assessment for 185 of the 208 neonates (88.9%). Data for analysis relates only to the final referral if the infant was referred more than once given that an infant referred twice could not possibly have died during the first referral event.
↵b Chi square = 37.3 with 2 df, P< .001; comparing “extremely sick” vs. combined (“not sick” and “moderately sick”), RR of fatal outcome = 8.61, 95% CI = 4.0–18.5.









{kind=link}
{kind=link}