


Figures & Tables
Figures
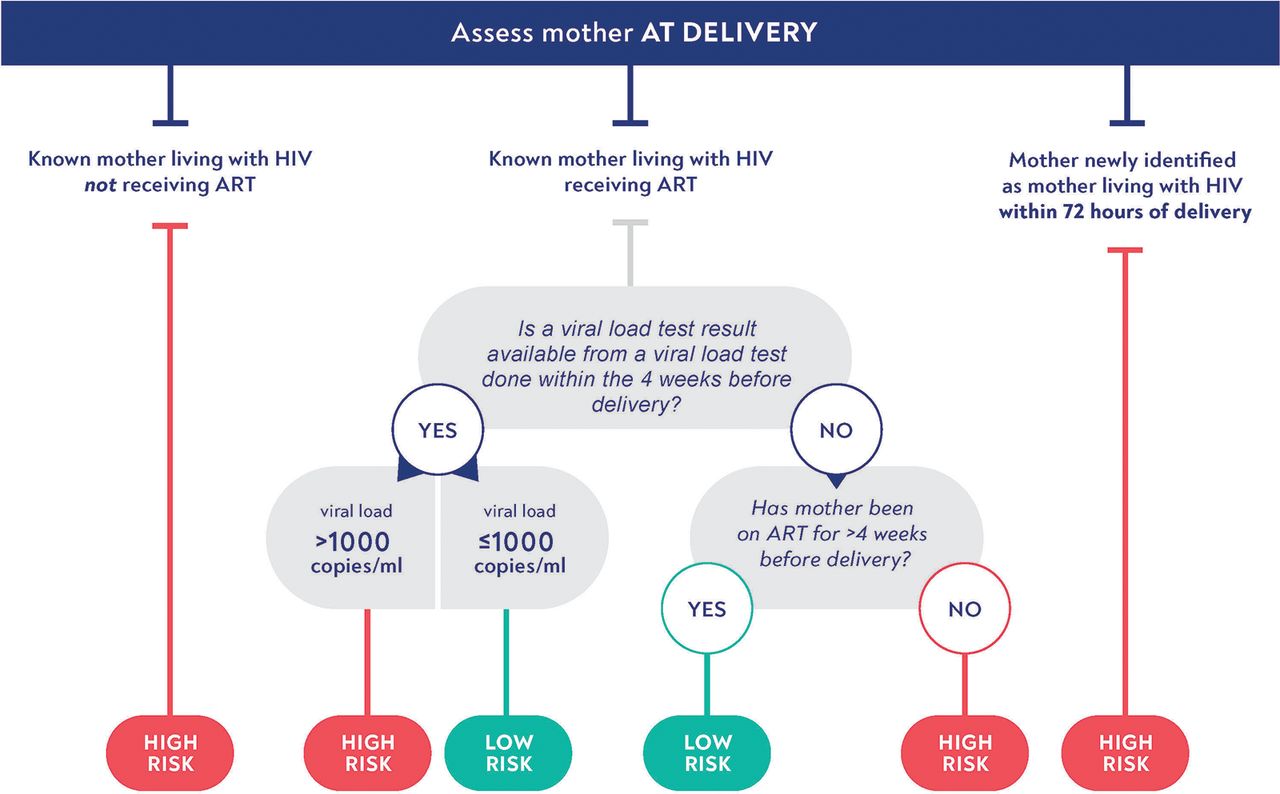
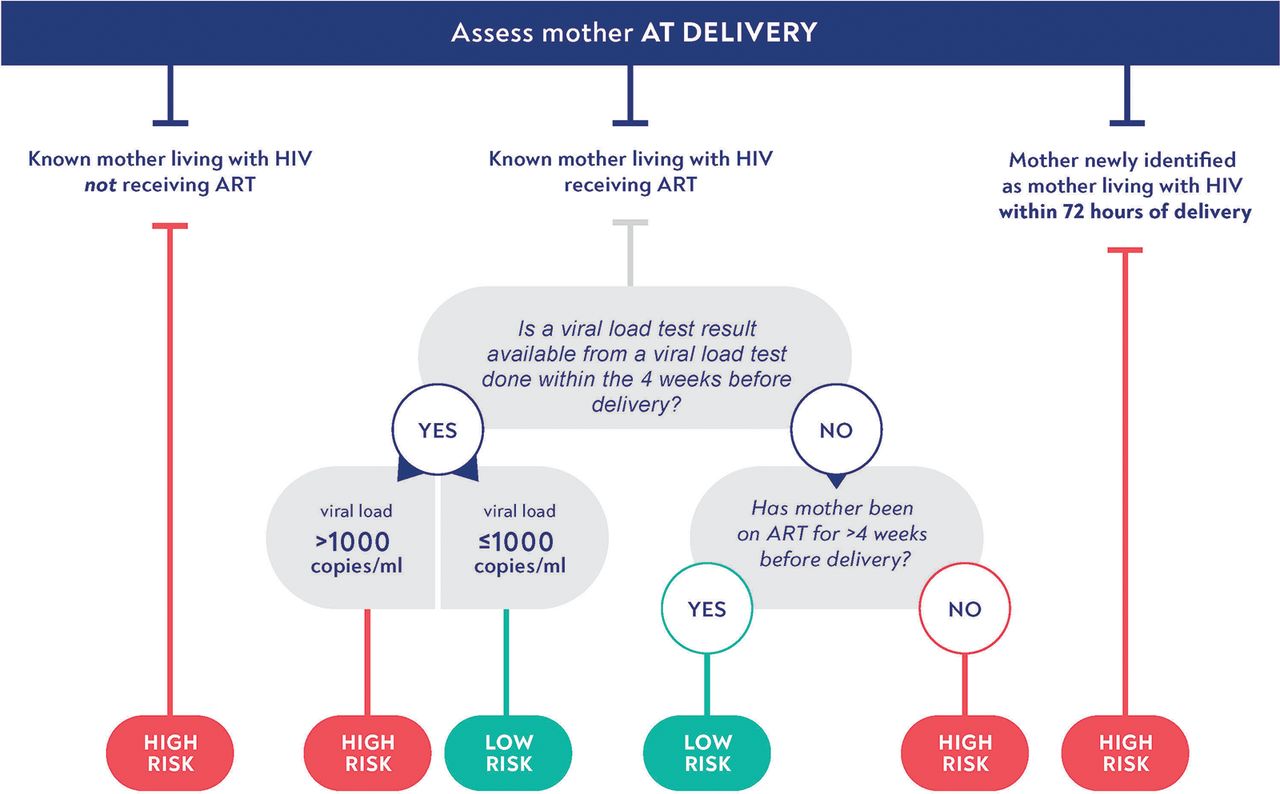
- FIGURE 1
Current Algorithm for HIV Transmission Risk Stratificationa
aAdapted from: World Health Organization’s Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach.5
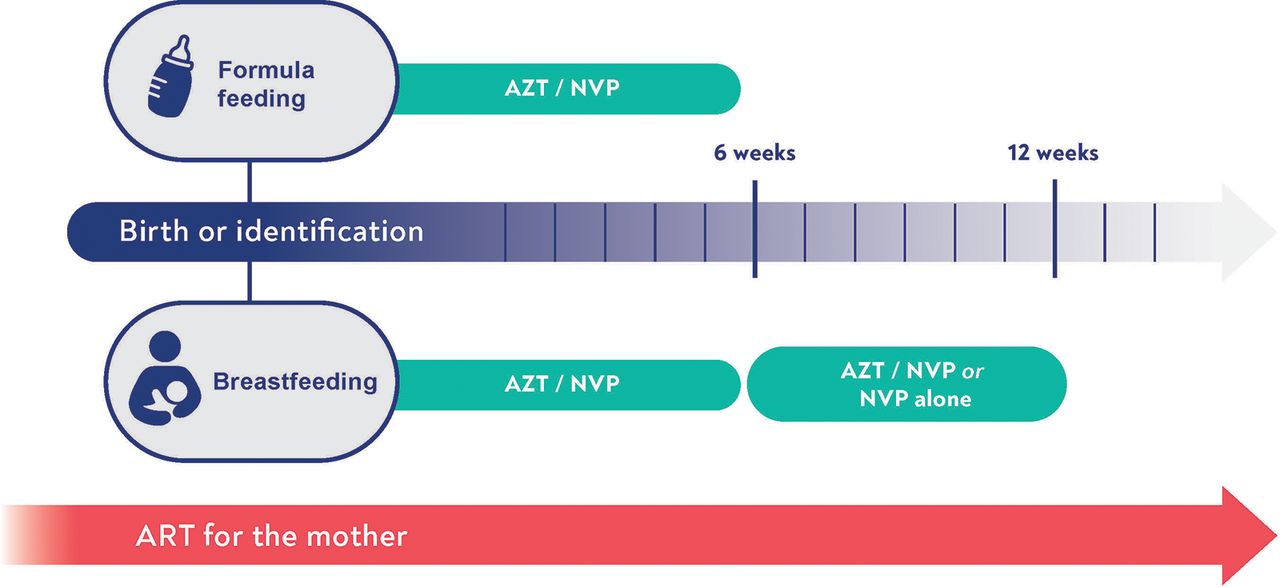
- FIGURE 2
Current Postnatal Prophylaxis Guidance for Infants at High Risk of HIV Transmissiona
Abbreviations: AZT: zidovudine; NVP: nevirapine; ART: antiretroviral treatment.
a Figure design based on guidance from: World Health Organization’s Consolidated Guidelines on HIV Prevention, Testing, Treatment, Service Delivery and Monitoring: Recommendations for a Public Health Approach.5
- FIGURE 3
Novel Approaches to Infant Postnatal Prophylaxis
Abbreviations: ALD, abacavir plus lamivudine plus dolutegravir tablets; ALL, abacavir plus lamivudine plus lopinavir-ritonavir granules; bNabs, broadly neutralizing antibodies; LA ARV, long-acting antiretroviral drugs; LR, low-risk situations; HR, high-risk situations.
a For premature babies, zidovudine and nevirapine should be used.


Tables
In Favor Against Risk of HIV acquisition is not uniform among exposed infants; different approaches are needed to address different scenarios; patient-centered approach tailoring response to individual infant. Risk may become more uniform (and low) in near future, with rapid scale-up of more potent, efficacious, and tolerable maternal treatment with dolutegravir. Low-risk infants avoid unnecessary antiretroviral drug exposure and the associated potential toxicities. A low rate of transmission persists even among low-risk infants, suggesting potential benefit from additional agents to all exposed infants. High-risk infants benefit from more aggressive management with multiple drugs/agents. No evidence exists to support the efficacy of multiple drug perinatal prophylaxis when mothers are on effective treatment, with studies performed in the era of dolutegravir-based treatment. Stratification aligns risk (toxicity): benefit (prophylaxis efficacy) of approaches with the transmission risk. Risk is difficult to assess and dynamic. Perinatal risk assessment depends on testing and medical records that are not always available. Over the duration of breastfeeding, individual maternal risk can change and can be difficult to assess without frequent visits and viral load testing. Stratified approaches optimize health system resource use, aligning cost of more intensive regimens with target population that will derive the most benefit. Risk assessment adds complexity and is itself resource intensive, requiring testing and visits for mothers. It can be challenging for health systems and clinics to stock and implement multiple regimens for infants. - TABLE 2.
Rationale for and Against Whether All Infants Should Receive Postnatal Prophylaxis While Breastfeeding
In Favor Against A large portion (∼50%) of vertical transmission currently occurs during the breastfeeding period. Studies have not shown that adding infant prophylaxis to effective maternal treatment further reduces transmission risk. Risk of transmission throughout breastfeeding is dynamic, with maternal viremia difficult to monitor or predict; maternal viremia during breastfeeding is common even among mothers who maintain suppression during pregnancy. More effective oral treatment with dolutegravir and new long-acting formulations offer the prospect of unprecedented coverage and durability of virologic suppression in breastfeeding women. Maternal adherence to treatment is difficult to sustain throughout the breastfeeding period; approaches to support nonadherent women to achieve viral suppression and to predict lapses in adherence are inadequate. Predictors of maternal nonadherence have been identified (including younger age, new HIV diagnosis, late presentation to care, and non-disclosure) and can be used to target additional prevention measures. Infants deserve resources and interventions that offer direct protection and do not rely on maternal treatment. Limited resources should focus on optimizing maternal adherence and access to good care. Routine infant care can serve as a platform to maintain infants on prophylaxis throughout breastfeeding. It is difficult to maintain infant prophylaxis over long periods of time; there is significant loss to follow-up by 1 year of life. New injectable and long-acting formulations limit the visibility of infants receiving prophylaxis and could reduce concerns about stigma. Providing prophylaxis to infants raises issues of disclosure of maternal infection status. Many mothers fall out of care, thus, interventions that do not depend on maternal clinic attendance are needed. New point-of-care viral load testing will make monitoring of mothers easier. Simplified, safer options that have potential for greater efficacy for postnatal prophylaxis are in development. Addressing underlying drivers of maternal treatment failure will benefit both the infant and the mother. Agent Potential Route and Frequency of Delivery Advantages Disadvantages Available now Dolutegravir Oral, daily Dispersible 5 mg tablet; broadly available with good supply chain; high resistance barrier; low toxicity. No evidence of efficacy for prevention. Dosing for infants aged younger than 4 weeks is not yet available; infections could lead to selection of drug resistance, jeopardizing use as treatment. Lamivudine Oral, twice daily Available in syrup and solid formulations; dosing available down from 32 weeks gestation; broadly available with good supply chain; low toxicity; demonstrated efficacy for postnatal prophylaxis. Low barrier to resistance. Lopinavir/ritonavir Oral, twice daily Available in liquid formulation and granules; demonstrated efficacy as postnatal prophylaxis. Twice daily dosing is less convenient. Persistent concerns about toxicity in neonates aged younger than 14 days and premature, possibly related to vehicle of liquid formulation. Abacavir Oral, once daily Well-tolerated in children, with fewer long-term side effects compared to zidovudine. No evidence of efficacy as prophylaxis; evidence of long-term toxicity in adults. In development pipeline Broadly neutralizing
antibodiesIntramuscular, every 1–2 months (maybe longer) Dosing for VRCO1, VRCO1LS, and VRC07-523LS is available; new class with high barriers to resistance and separate pathway from current treatments; easy to dose across growth periods; well tolerated; no drug-drug interactions. Appeal of injections to some settings: doesn’t rely on adherence to daily oral, fewer adherence/stigma issues compared to oral medications kept at home. Current options must be combined to optimize antiviral effects; efficacy for prevention indication still needs to be demonstrated; requires cold chain and site capacity to deliver. Biosimilar production will be a significant challenge. Islatravir Oral, monthly Could be delivered in clinics, facilitating dose adjustments, or at home. New class with high barriers to resistance and separate pathway from current treatments. Appeal of injections to some settings: doesn’t rely on adherence to daily oral, fewer adherence/stigma issues compared to oral medications kept at home. Drug development halted due to evidence of lymphocyte toxicity (ongoing investigation may allow continuation of the drug development program in the future). Lenacapavir Subcutaneously, every 3–6 months As a new drug class, lower risk for interaction with maternal or infant treatment; surmounts issues of adherence to oral regimens. May need more frequent dosing during first year of life to accommodate growth. Cabotegravir Intramuscular, once every 1–2 months Appeal of injections to some settings: doesn’t rely on adherence to daily oral, fewer adherence/stigma issues compared to oral medications kept at home. Pharmacokinetics will be challenging, especially for infants aged younger than 4 weeks and premature infants. Infections could lead to selection of resistance, compromising other agents like dolutegravir. Generic production will be a challenge in the immediate future.









{kind=link}
{kind=link}
{kind=link}
Statistics from Altmetric.com
Jump to section
- Article
- INTRODUCTION
- WHAT IS THE EVIDENCE BASE FOR CURRENT APPROACHES TO POSTNATAL PROPHYLAXIS?
- WHAT ARE THE CHALLENGES SPECIFIC TO STUDYING PHARMACOKINETICS AND DETERMINING DOSING FOR NEONATES?
- WHAT CAN WE LEARN FROM STUDIES OF HIV ANTIRETROVIRAL PROPHYLAXIS IN ADULTS ABOUT TARGET PRODUCT PROFILES?
- WHAT IS THE POTENTIAL ROLE OF PASSIVE IMMUNIZATION IN POSTNATAL PROPHYLAXIS?
- DO POSTNATAL PROPHYLAXIS STRATEGIES NEED TO BE RISK STRATIFIED?
- SHOULD ALL INFANTS RECEIVE POSTNATAL PROPHYLAXIS WHILE BREASTFEEDING?
- WHAT ARE POTENTIAL APPROACHES TO POSTNATAL PROPHYLAXIS IN THE NEAR AND FAR FUTURE?
- CONCLUSION
- Funding
- Disclaimer
- Author contributions
- Competing interests
- Notes
- REFERENCES
- Figures & Tables
- Info & Metrics
- Comments
Related Articles
Cited By...
- No citing articles found.