


Figures & Tables
Figures
- FIGURE 1
PRISMA Flow Diagram37 for a Rapid Review of CHWs as Vaccinators
Abbreviations: CHW, community health worker; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
- FIGURE 2
Countries With Community Health Workers Who Administer Vaccines
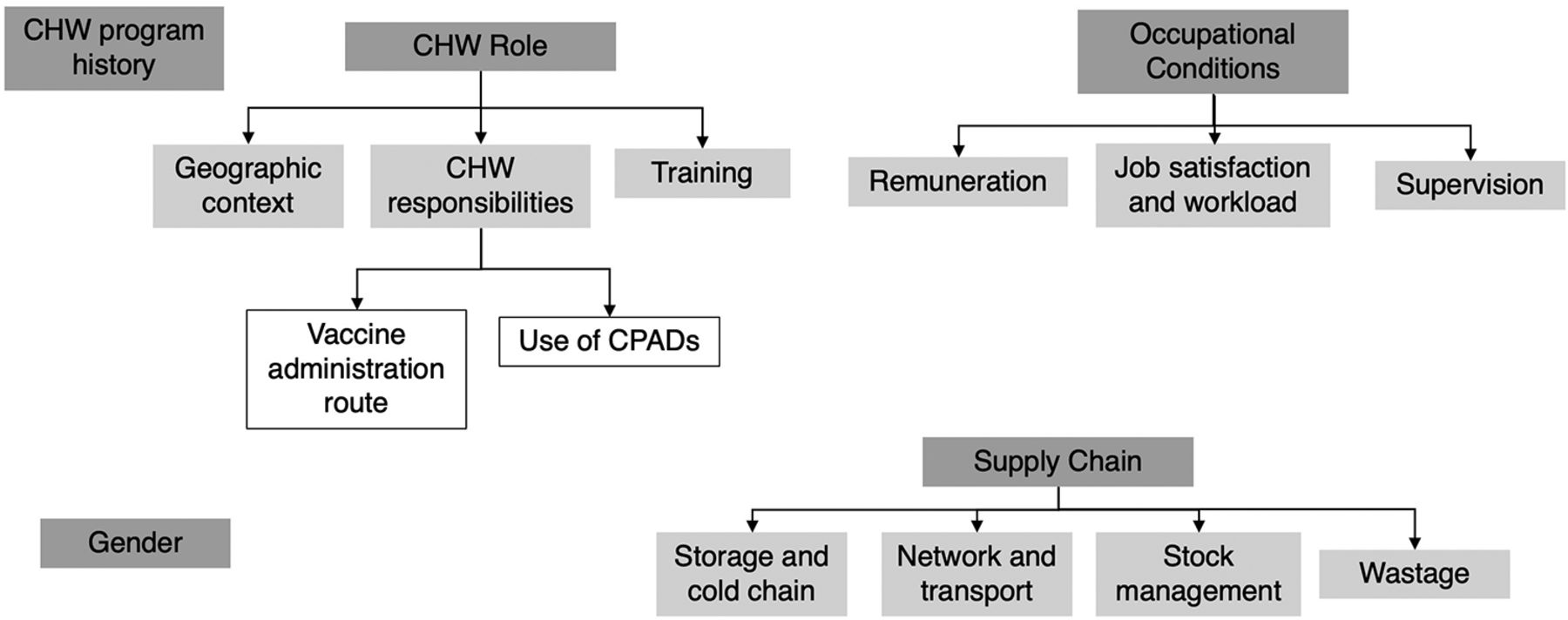
- FIGURE 3
Health Systems Categories Related to CHWs as Vaccinators
Abbreviations: CHW, community health worker; CPAD, compact prefilled auto-disable device.
- FIGURE 4
Remuneration for CHWs Who Administer Vaccines
Abbreviation: CHW, community health worker.



Tables
- TABLE 1.
CHW Cadres That Administered Vaccines and Related Health Systems Factors, by Country
Country,Vaccinating CHW Cadre, Vaccine Type,Program Type Categories Program History CHW Role Supply Chain Occupational Conditions Gender Afghanistan, TBA, injectable, project or temporary campaign NR Geographic context: Door-to-door community campaigns.51
Responsibilities: Tetanus toxoid vaccination campaigns using CPADs.51
Training: NRStorage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: NR
Job satisfaction and workload: NR
Supervision: NRNR Bangladesh, HA, injectable, established program Initially served as vaccinators or supported malaria control. 1995: expanded to additional preventative health and curative duties. Recruited, trained, and supervised within formal government health system.59 Geographic context: Rural areas.59
Responsibilities: Provide women and children immunizations, vitamin A supplementation, and oral rehydration salts; detect and treat TB, diarrhea, malaria, and pneumonia.47,59 Split time between community clinics and home visits.59 Other CHW cadres: family welfare assistants, community health care providers, and CHWs employed by NGOs.59
Training: Requisite 10 years’ schooling; 21 days’ preservice training, on-the-job training.59Storage and cold chain: Porters transport the immunization supplies from cold storage centers to the union level.47
Network and transport: Travel to sites using their own motorcycles or bicycles; given a transport allowance.47
Wastage: NR
Stock management: NRRemuneration: Paid full-time workers47: government salary US$135–327/month.59
Job satisfaction and workload: NR
Supervision: Assistant health inspectors supervise 3 HAs.59Male or female. Historically been male due to the perception that men are more flexible and mobile and the cadre is currently mostly male.47,59 Brazil, community health agent, injectable, established program Started with promoting immunization, breastfeeding, and oral rehydration solution. Expanded into national public health program. Have an integral role in the system's family health teams to provide primary health care to specific catchment areas.59 Geographic context: Mainly outside health facility.59
Responsibilities: Provide preventative and curative services and education (e.g., immunizations, perinatal care, and screening and treatment of infectious and chronic diseases).59 Work closely with their family health team (i.e., 4–6 community health agents, nurses, doctors, dentists.)59
Training: 1,200 hours formal didactic and field activities.59Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Paid, full-time workers: government salary US$226–380/ month.59
Job satisfaction and workload: Some feel underval-ued by teams, frustrated by low salary and low status, no clear path for career advancement.59
Supervision: Supervised by nurses on family health team but often missed due to lack of supervising nurses’ time.59NR China, village-based health worker, injectable, project or temporary campaign Administration of hepatitis B vaccines was outside usual role of the village-based health workers.48,67 Geographic context: Rural areas where many children are born at home.48,67
Responsibilities: Administered hepatitis B vaccines using CPADs to infants delivered outside hospital system.48,67
Training: NRStorage and cold chain: CPAD stored at room temperature outside cold chain in the homes of village-based health workers or in clinics.48,67
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: NR
Job satisfaction and workload: NR
Supervision: NRNR DRC, volunteer vaccinator, OPV only, established program Polio vaccine campaign began in 1995 in response to outbreak that involved volunteer vaccinators.49 Geographic context: Most remote areas of the country.49
Responsibilities: Deliver OPV and may also deliver other preventative health services and supplies.49
Training: NRStorage and cold chain: Transport vaccines in vaccine boxes.49
Network and transport: Must travel long distances carrying vaccine boxes, over challenging terrain using canoes, cars, motorcycles, and bicycles, and on foot.49
Wastage: NR
Stock management: NRRemuneration: NR
Job satisfaction and workload: NR
Supervision: NRNR Ethiopia, HEW, injectable, established program Formally recognized cadre within government health system with high levels of political support.59 Some reports of administrative and managerial challenges.61 Geographic context: Health posts and on specific days at locations around health posts’ catchment area.38,47,50,59,61
Responsibilities: Preventative services (e.g., health education, counseling, FP, and immunization); basic curative services (e.g., first aid and chronic disease management)38,40,41,47,50,59,61; administer injectable contraceptives.40,50,61 Work closely with women's development army (volunteer CHWs that expand HEW reach)59 and health center staff.40,59
Training: Requisite completion of grade 10, 1 year preservice training38,41,50,59; in-service training every 2 years.59Storage and cold chain: Federal MOH provides medical equipment, supplies, vaccines and cold chain equipment.40 Vaccines transported in vaccine carriers or cold boxes from the health center to outpost. Unused doses brought back at the end of the day.47
Network and transport: HEWs often travel on foot and sometimes use motorcycles. HEWs are supposed to receive reimbursement for transport but this is sometimes not provided due to shortages in funds.47
Wastage: NR
Stock management: Challenges with shortages of drugs, medical supplies, and equipment.59,61Remuneration: Government salary US$84/month.38,40,59 Can obtain salary increases through additional training and exams.59 Per diems and transport reimbursements may not be provided due to lack of funds.47
Job satisfaction and workload: HEWs may be overburdened due to increasing numbers of tasks assigned.59 Lack of a clear career trajectory for HEWs as a challenge.59
Supervision: Regional health bureaus and district health offices provide support and leadership.40 Supervised by health center staff associated with their health post, and sometimes accompanied on vaccination outreach by a health center supervisor.47,59 HEW program evaluations identified lack of regular supervision,61 but other reports have noted supervision to be regular.59Women aged over 18 years, usually work at health posts in pairs.50,59 Ghana (1 of 2), CHO/ CHN, injectable, established program First unpaid CHVs provided immunization and other preventative health tasks. Government transitioned to a paid, more highly trained CHO/CHN cadre.59 Geographic context: Villages and based out of health posts; also engage in outreach services within their zone.59
Responsibilities: Preventative services to their CHPS zone (e.g., childhood routine immunizations)59 Administered injectable contraceptives.59 CHOs supervise CHVs within their zone.59
Training: All CHOs are first trained as CHNs: 2 years of didactic and field training, with periodic in-service training.59 CHNs become CHOs after completing training and orientation in community engagement and mobilization and being posted to a health post.59Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Full-time MOH salary US$140/month. Paid leave and opportunities for paid educational leave.59
Job satisfaction and workload: NR
Supervision: Receive facilitative supervision focused on mentoring and problem solving from the GHS from a public health nurse, physician assistant, or designated CHPS coordinator.59NR Ghana (2 of 2), TBA, injectable, project or temporary campaign GHS had initial concern about TBAs delivering tetanus vaccines (i.e., this would encourage TBAs to work outside their general scope of practice outside the campaign context, especially as TBAs might benefit financially by offering injection services as they are not officially salaried by the GHS). This was assuaged by ensuring that the training for TBAs to use a CPAD addressed these concerns.45 Geographic context: Rural area.45
Responsibilities: Delivered tetanus toxoid injections to women of childbearing age using a CPAD.45
Training: Before campaign, the TBAs had little or no formal education, although some had prior training in delivering other health care services.45 TBAs received training from a few hours to 2 days in delivering the tetanus vaccine using the CPAD.45 TBAs reported feeling confident in their ability to safely and correctly use CPADs.45Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Those who participated in the tetanus campaign were unpaid.45
Job satisfaction and workload: Felt their community status was increased through involvement in the tetanus campaign.45
Supervision: Supervised during campaigns but some delivered vaccine independently.45NR India, ANM, injectable, established program ANMs are official roles within the government health system.59 Initially, the ANM role focused on perinatal care and ANMs were expected to stay at the subcenter to conduct deliveries.52 The role expanded to be a “multipurpose worker” which included more general maternal and child preventative care along with routine immunizations.52 The midwifery component of the role was deprioritized, and ANMs now focus on FP and immunization.52,59 Geographic context: Posted at subcenters but many immunization activities are conducted in the community and require the ANMs to travel to villages to conduct outreach sessions with target populations.52,59,60
Responsibilities: Deliver preventative and curative interventions (e.g., routine immunizations, FP, and maternal and child health programming).59,60,62,64,66 ANMs provide care at the subcenter level, conduct home visits, and participate in village health days.59,60,62,66 ANMs work closely with other cadres of CHWs, especially AWWs and ASHAs, which both play significant roles in delivery of immunization services, supporting organization of village health days, and community mobilization and education to promote immunization efforts.59,62,64,66
Training: Must be aged between 17–35 years and have finished 12 years of school to apply to the ANM training program.59 24 months of preservice training.59 Some reports found ANMs expressed the need for additional training on a variety of topics including new immunizations.62Storage and cold chain: Experience cold chain challenges when conducting vaccinations, including storing vaccines in their domestic refrigerators and limited cold chain staff available for support.55 Reports also note a need for additional training in cold chain management and maintenance for ANMs to ensure vaccine potency especially in outreach settings.55
Network and transport: Report transportation challenges (e.g., limited public transportation and rough terrain).62
Wastage: NR
Stock management: ANMs report vaccine shortages as a barrier to administering and promoting vaccines.64Remuneration: Salaries vary by state, but are paid a government salary of approximately US$280 per month.59
Job satisfaction and workload: Considered “multipurpose workers” whose scope requires them to balance time between home visits, health center, and community immunization campaigns.52,64 ANMs are also often required to supervise the health center.59
Supervision: Lady health visitors supervise ANMs, and there is one lady health visitor for every 6 subcenters.59 ANMs can become lady health visitors once they have 5 years of experience and after taking a 6-month training course.59 However, reports indicate some ANMs do not feel they receive meaningful supervision.59Must be female to apply to the training program.59 Another male cadre of CHWs, multipurpose health workers, sometimes accompany ANMs to remote areas and provide support with transportation. Sometimes ANMs do not feel safe traveling to certain areas without the support of a male multipurpose health worker.62 ANMs have been verbally harassed, had stones thrown at them, and been sexually assaulted after being called to village homes, and some refuse to attend house calls at night due to security concerns.59 Indonesia (1 of 2), kader, injectable, established program The community sessions run by the kaders first focused on basic nutrition, growth monitoring, and FP.59 The MOH later added additional functions (e.g., to expand immunization coverage and provide curative services).59 Reports suggest many kaders have given up their roles out of a need to pursue paid employment, and that many of the community sessions no longer occur.59 Geographic context: Host sessions at a central location in the community.59
Responsibilities: Collaboratively run a community health post called a posyandu.59 Hold monthly sessions on maternal and child health education and preventative services (e.g., immunization and resupply of FP products).59 Supported by local health center staff (i.e., doctors, nurses, and midwives).59
Training: Less than a week of formal training; many skills acquired through experience.59Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Volunteers, not compensated formally.59 May receive reimbursements for travel expenses and informal compensation (e.g., medical treatment).59
Job satisfaction and workload: Seen to be a highly esteemed community role and may receive awards for years of service.59
Supervision: Supervised by primary care doctors, nurses, and midwives from the nearby health facility.59 At least 1 of those staff members is present for community session run by kaders.59The majority are female, but this is not a requirement.59 Indonesia (2 of 2), community midwife, injectable, established program Trials of community midwives administering the birth dose of hepatitis B were ongoing, but there were issues managing multidose vials and disposable syringes.51 1995: Community midwives piloted use of CPADs to deliver hepatitis B outside the cold chain. 2003: Expanded to target all births in Indonesia.51 Geographic context: Home visits in villages.51
Responsibilities: Deliver birth dose of hepatitis B using a CPAD.51
Training: NRStorage and cold chain: The hepatitis B dose using CPAD able to be stored outside cold chain in midwives’ homes.51 Midwives given safety boxes for disposing used CPADs.51
Network and transport: Already received travel allowances to perform neonatal home visits before adding hepatitis B injection requirement.51
Wastage: CPAD helped prevent wastage.51
Stock management: NRRemuneration: Travel reimbursement to conduct home visits.51
Job satisfaction and workload: NR
Supervision: NRNR Iran, behvarzes, injectable, established program Government established a lay health cadre to administer immunizations and manage communicable diseases comprised of men with at least 6 years of general education who were provided with a short additional training course.59 Government piloted several different models for providing public health care to rural areas, which was eventually developed into the health house model staffed by behvarzes beginning in 1979.59,63 Geographic context: Rural areas.59,63
Responsibilities: Provide a range of preventative and curative community health services for adults and children (e.g., routine immunization) and engage in community mobilization and engagement.59,63 1–2 behvarzes run health houses (small rural health outposts).59 Behvarzes partner with a second behvarz at health house.59,63
Training: Must have completed 12 years of general education followed by 2 years’ didactic and practical training.59 More recently, many also have an undergraduate degree.59 They are offered monthly refresher courses.63Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Government salary ∼ US$350/month (may increase based on performance).59 Additional incentives (e.g., training funds, awards, celebrations, and loans).63 Free training; funds for transportation, food, and accommodation during 2 years of training.59
Job satisfaction and workload: NR
Supervision: Supervised by higher-level staff from the local comprehensive health centers who regularly visit the health houses.59,63Both men and women are eligible; health houses often staffed by 1 man and 1 woman from each village.59,63 Priority is given to workers from the community in which the health house is located or to women whose husbands have a permanent position in the village.59 Kenya (1 of 2), CHW, injectable, project or temporary campaign NR Geographic context: NR
Responsibilities: Provide maternal and child-focused preventative and basic curative services including childhood immunization and family through community-based nonprofit Lwala Community Alliance.46
Training: NRStorage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Salaries paid by Lwala Community Alliance of US$200/month and includes supplies and supervision, although it’s unclear what percentage of that amount goes directly to the CHW.46
Job satisfaction and workload: NR
Supervision: NRNR Kenya (2 of 2), CHV, OPV only, project or temporary campaign NR Geographic context: In an effort to reach nomadic families and those living in remote settlements, CHVs administered OPV to children at boreholes and water access points in rural communities.39
Responsibilities: As part of an oral polio SIA, CHVs were trained to administer OPVs to children in remote areas.39 Social mobilization was led by members of the nomadic communities, while CHVs and health workers administered the OPVs.39
Training: NRStorage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: NR
Job satisfaction and workload: NR
Supervision: NRNR Malawi, HSA, injectable, established program 1960s: Temporary lay health cadre created to provide smallpox vaccines.
1973: New cadre created to address cholera and was later expanded to the role of the HSA to focus on health promotion and preventive services.23,59 Although this was not the case for many years, HSAs are an officially recognized cadre with legal support from the MOH and considered to play an important role in public health system.58,59Geographic context: Health centers, outreach clinics, and during national immunization days organized to reach families in remote areas.53,58,59,65
Responsibilities: Provide community engagement, social mobilization, and preventative public health services for adults and children.23,53,56–59,65 HSAs are one of the main providers of immunization.53,56,58 Engage in limited basic curative tasks23,59 and administer injectable contraceptives.23 Collaborate with teachers to provide education and promote HPV vaccines among young women.57 Malawi has several cadres of CHWs: senior HSAs, CHNs, community midwife assistants, and assistant environmental health officers, and CHVs.23 Work closely with community leaders, community organizations, and volunteers.59
Training: Must be aged at least 19 years, have completed 4 years of education, and speak English and the local language.59 12 weeks’ didactic and fieldwork training56,59 and may receive ongoing refresher trainings.59 May have limited opportunities for continuing education.58Storage and cold chain: NR
Network and transport: Often have to travel long distances to reach outreach clinics to deliver immunizations, and many have to walk as they do not have bicycles provided by the health system.53,58 Even for HSAs who are provided with bicycles, they may not be fully functional, or may not work on the hilly terrain they have to travel on.53,58 HSAs may be required to pay for bicycle repairs themselves.58
Wastage: NR
Stock management: Often work without gloves due to limited supplies.58Remuneration: Receive a government salary of approximately US$63 per month, along with per diems for trainings and events, and some nonfi-nancial incentives such as clothing and a bicycle.59 There are some concerns about low remuneration.58,59
Job satisfaction and workload: Overburdened with tasks due to balancing requirements related to immunization with other community engagement needs.23,53,57–59 There is concern that some HSAs have taken on additional curative tasks without adequate training.23 HSA vaccination targets are used as performance measures, which can place pressure on HSAs.58 When schools closed during the COVID-19 pandemic, HSAs did some social mobilization tasks to promote HPV vaccines.57 HSAs have limited opportunities for career advancement and continuing education and limited incentives and remuneration.58,59
Supervision: Supervised by senior HSAs monthly and assistant environmental health officers quarterly.59 There is some concern that HSAs do not have adequate supervision.23,53NR Mali, TBA, injectable, project or temporary campaign There was initially some pushback from policymakers against TBAs administering tetanus toxoid injections using a CPAD independently as part of routine immunization, so TBAs first administered the vaccine under close supervision by health care personnel in a community campaign setting.45 Geographic context: Door-to-door in communities in rural areas.45,51
Responsibilities: Administer tetanus toxoid injections using a CPAD.45,51
Training: Limited or no previous education, and many received some training on delivery of health care services.45 Received between a few hours to 2 days training on using a CPAD.45,51Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Not paid but provided with transportation and food during the training on the use of the CPAD.45
Job satisfaction and workload: NR
Supervision: Initially closely supervised by health care personnel when administering tetanus toxoid in community campaigns.45NR Nepal, AHW, injectable, established program Nepal MOH has had several iterations of CHW cadres to address rural health needs beginning with VHWs who were primarily male and whose main task was to administer immunizations.47,59 VHWs transitioned into AHWs, either replaced as they retired or given additional training to meet AHW requirements.47,59 Geographic context: Work from health posts located in villages.59
Responsibilities: Administer vaccines.47,59 Partner with other health worker cadres (e.g., ANMs and part-time female community health volunteers),59 who primarily engage in education and social mobilization (e.g., promoting immunizations).59
Training: 15–18 months of preservice training.47,59Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Paid government workers.59
Job satisfaction and workload: NR
Supervision: NRNR Niger, agent de santé communautaire, injectable, established program MOH initially created CHW cadres with limited training focused on education and emergency response. 2000: government expanded focus on providing rural health services and then introduced the agent de sante communautaire and relais volunteer roles.59 Geographic context: Stationed at health posts located in communities at least 5 km from nearest hospital or health center.59
Responsibilities: Provide preventative services (e.g., immunizations and FP), some basic curative care,59 and administer injectable contraceptives.59 Work closely with and supervise relais volunteers, volunteer cadre based at same health post but who focused on health promotion and community mobilization for immunization campaigns outside the health posts in villages.59
Training: Must have completed primary school education, but many have a higher level of education.59 6 months of preservice training.59Storage and cold chain: Get supplies from health center associated with their health post.59
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Salary ∼ US$100/month.59
Job satisfaction and workload: NR
Supervision: Supposed to be supervised by staff members from health center, but this may not occur regularly.59Generally male.59 Nigeria, CHEW or junior CHEW, injectable, established program CHW cadres began in 1970s with 2 different regional approaches, one focused on VVHWs coordinated by NGOs and the other CHEWs coordinate by the government.59 The public health systems have been restructured to establish village health posts that CHEWs work from, and their training evolved to focus around an extensive book of “standing orders” which outlines their scope of work.59 The MOH recently required that all VVHWs be reclassified as community health influencers and promotors service (CHIPS) agents, to standardize training and reduce the silos between different programs.59 Geographic context: Health centers at least 5 km from the closest government health facility and sometimes in community.47
Responsibilities: CHEWs and junior CHEWs provide preventative services (e.g., immunizations) and some basic curative services.47,59 VVHWs or CHIPS agents focus on health promotion and education.59 CHEWs work closely with and supervise the CHIPS agents who are based out of the same facility as them.59
Training: CHEWs: 3 years of pre-service training; junior CHEWs: 2 years.47,59Storage and cold chain: For health centers with refrigerators, CHEWs pick up vaccines every month, but for those without, CHEWs pick up vaccines on immunization service provision day.47 They transport vaccines in vaccine carriers or cold boxes.47
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Government employees ∼ US$281/month.59
Job satisfaction and workload: CHEWs were supposed to split their time between working from the health center and working out in the community, but due to staffing shortages and increasing workload, they are often unable to leave the health centers to work in the community, and some services were offered infrequently.47,59 Due to a lack of clinicians available in rural areas, they may be under pressure to focus on curative needs.59
Supervision: CHEWs supervised by staff from nearby health facility.59NR Pakistan, LHW, injectable, OPV only in some provinces, established program Launched in 1994 and focused on FP and primary health care. Expanded to support large campaigns to address immunization and some management of communicable diseases.59 2001: MOH approved a policy allowing LHWs to administer injections. 2008: approved policy allowing LHWs to participate in campaigns as EPI vaccinators.21 However, LHWs may only be allowed to administer vaccines in certain provinces.44 Geographic context: May work from a local clinic, from their homes, and door-to-door visiting families.43,44,54,59 They may travel to different communities as part of large immunization campaigns.54 LHW services focus on rural and poor urban areas.59
Responsibilities: Provide preventative services focused on maternal and child health and participate in vaccination efforts as social mobilizers, educators, and vaccinators.21, 43,44,54,59 LHWs play key role in delivering polio vaccines through large campaigns.43,54 Their exact scope of work differs between provinces.44 Administer injectable contraceptives.21,59 Collaborate with TBAs and midwives and refer patients to health centers for higher levels of care.59 May share vaccination sessions with other vaccinators,21 although there may be some tension between LHWs and vaccinators.44
Training: To apply, LHWs must have at least 8 years of education and be aged 18–50 years.59 15 months of didactic and fieldwork training and yearly refresher trainings.59 LHWs receive extensive training specific to vaccination, and many feel confident administering intramuscular injections.21 There may be some gaps in LHW training related to specific vaccines.44Storage and cold chain: Obtain vaccines primarily from health centers and other vaccinators.21 They are not provided with vaccine carrier boxes or transportation support and must make their own arrangements for cold chain management.21
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Government salary ∼ US$90–180/month,43,59 although there are concerns that remuneration is not adequate and unreliable.43
Job satisfaction and workload: Some concern the addition of immunization to their standard tasks may overload LHWs.44,54 Some LHWs have advocated for increased benefits and boycotted participating in vaccine activities due to experiences of violence in communities and not being paid for several months.59
Supervision: LHWs are associated with a public health clinic and are supervised by lady health supervisor from that clinic at least once per month.59 LHWs participating in immunization sessions under EPI may also be supervised by area vaccinators and the district health management team.21LHWs are all women,21,43,44,54,59 and preference is given to married applicants.59 Government deploys LHWs, as a cadre of women, in vaccination campaigns as male staff will often not be admitted into some parts of the family home.54
LHWs sometimes travel away from their communities to participate in campaigns in areas with few LHWs.54 If female LHWs are traveling unaccompanied by their husbands, they may be perceived poorly by the community including being targets of verbal and physical abuse and being refused entry into family homes.54 LHWs were targeted by militant groups while participating in polio vaccine campaigns.43,59 LHWs are sometimes offered police escorts, but some decline them as they feel it draws attention and makes them more of a target.43Papua New Guinea, village health volunteer, injectable, project or temporary campaign This program was organized by an NGO in partnership with local communities and local government.45 Some village health volunteers were nervous about the additional responsibility related to their new role as vaccinators, so were provided with a copy of a formal letter authorizing them to administer this vaccine from the department of health.45 Geographic context: Infants’ homes and at local clinics in rural areas.45
Responsibilities: Administered the birth dose of hepatitis B vaccines using CPADs to infants within the first 24 hours of birth and45 delivered other preventative services (e.g., education and distribute medications).45
Training: 6 weeks of training and45 1-day training on delivering hepatitis B vaccine using a CPAD.45Storage and cold chain: NR
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: Unpaid volunteers but during training given accommodation, food, small stipends, and commodities (e.g., soap and salt).45
Job satisfaction and workload: Addition of vaccinating task increased motivation to visit infants immediately after birth.45
Supervision: Supervised by project officer every 1–3 months.45Male and female.45 United States,
CHA/P, injectable, established programNR Geographic context: Rural communities in Alaska.42
Responsibilities: Provide health education and promotion, preventative services (e.g., immunizations), and interventions in emergency settings.42 CHA/Ps may be the only health care worker in their community.42
Training: 3–4 weeks.42Storage and cold chain: Have some limitations on their refrigeration capacity at clinics and are unable to store certain vaccines such as the varicella-zoster vaccine due to not meeting the cold chain requirements.42
Network and transport: NR
Wastage: NR
Stock management: NRRemuneration: NR
Job satisfaction and workload: NR
Supervision: NRNR Zambia, CHA, injectable, established program CHW cadres were initially not formally regulated, had many different titles, were trained for different lengths of time by different organizations, and had different scopes of work.59 Zambia then chose to formalize a paid CHW cadre, partially based on Ethiopia’s HEW cadre.59 Geographic context: Supposed to split their time between health posts and community.59
Responsibilities: Provide both preventative and some basic curative services including childhood immunizations.59 Work closely with other health posts staff (e.g., nurses, environmental health technicians, community development assistants, and social welfare volunteers who focus on education).59
Training: Applicants much have completed at least 12 years of education and be aged 18–38 years.59 1 year of preservice training.59Storage and cold chain: NR
Network and transport: CHAs experience transportation challenges.59
Wastage: NR
Stock management: Experience unreliable supplies of medication.59Remuneration: Government salary ∼US$250/month (includes civil servant benefits).59 Given uniform and some equipment (e.g., bicycle).59
Job satisfaction and workload: Due to staff shortages, CHAs are often required to manage care needs at the health posts and struggle to prioritize community-level work outside the health post.59
Supervision: Supervised by health staff either at health post or nearest associated health facility.59 Supervision is supposed to occur monthly in community but is often deprioritized and rarely happens.59Women are given preference during recruitment process.59 Abbreviations: AHW, auxiliary health worker; ANM, auxiliary nurse midwife; ASHA, accredited social health activist; AWW, anganwadi worker; CHA, community health assistant; CHA/P, community health aide/practitioner; CHEW, community health extension worker; CHN, community health nurse; CHO, community health officer; CHPS, Community-Based Health Planning and Services; CHV, community health volunteer; CHW, community health worker; CPAD, compact prefilled auto-disable device; DRC, Democratic Republic of the Congo; EPI, Expanded Programme on Immunization; FP, family planning; GHS, Ghana Health Service; HA, health assistant; HEW, health extension worker; HPV, human papillomavirus; HAS, health surveillance assistant; LHW, lady health worker; MOH, ministry of health; NGO, nongovernmental organization; NR, not reported; OPV, oral polio vaccine; SIA, supplementary immunization activity; TBA, traditional birth attendant; VHW, village health worker; VVHW, volunteer village health worker.
Country Community Health Worker Cadre Program Type Vaccine Administration Route Category of Vaccines Administered Established Program Project or Temporary Campaign Injectable Oral All Routine Immunizations 1 Specific Immunizationa Afghanistan Traditional birth attendant51 X Xb,c X Bangladesh Health assistant47,59 X X X Brazil Community health agent59 X X X China Village-based health workers48,67 X Xc X Democratic Republic of the Congo Village volunteer49 X X X Ethiopia Health extension worker38,40,41,47,50,59,61 X X X Ghana Community health officer59 X X X Traditional birth attendant45 X Xc X India Auxiliary nurse midwife52,55,59,60,62,64,66 X X X Indonesia Kader59 X X X Community midwives51 X Xc X Iran Behvarzes59,63 X X X Kenya Community health worker46 X X X Community health volunteer39 X X X Malawi Health surveillance assistant23,53,56–59,65 X X X Mali Traditional birth attendant45,51 X Xc X Nepal Auxiliary health worker47,59 X X X Niger Agent de santé communautaire59 X X X Nigeria Community health extension worker47,59 X X X Pakistan Lady health worker21,43,44,54,59 X X X X Papua New Guinea Village health volunteer45 X Xc X United States Community health aide/practitioner42 X X X Zambia Community health assistant59 X X X ↵a Trained as vaccinators to administer 1 specific vaccine (e.g., only hepatitis B vaccines).
↵b An X indicates clear affirmative evidence is available in documents included in review; a blank cell indicates no information was available in included documents.
↵c Use of a compact prefilled auto-disable device.
Supplemental material
- Supplements -
Supplements
- Supplements -









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Statistics from Altmetric.com
Jump to section
Related Articles
Cited By...
- No citing articles found.