


ABSTRACT
Introduction:
Community health workers (CHWs) could expand immunization access in under-reached communities by administering vaccines. This rapid review identifies countries where CHWs administered vaccines and synthesizes health systems factors that may contribute to or detract from the feasibility of CHWs administering vaccines.
Methods:
We conducted a rapid review of peer-reviewed literature from 3 databases and gray literature identified through web searches and by CHW subject matter experts. We treated extracted data on conditions related to vaccine administration by CHWs as qualitative data and conducted deductive content analysis.
Results:
We retained 32 documents from 497 initial records and identified 23 CHW cadres that vaccinated in 20 countries, ranging from long-established national programs delivering routine immunizations to pilot projects delivering 1 specific vaccine. CHWs who vaccinate face the following challenges: (1) inadequate supply chain training, (2) inadequate cold chain equipment, (3) transportation for supplies and to communities, (4) heavy existing workload, (5) inadequate or irregular remuneration, (6) inadequate or irregular supervision.
Conclusion:
To improve immunization coverage in underimmunized and zero-dose communities, countries where CHWs vaccinate should provide CHWs with adequate remuneration, supervision, supply chain support and management, and formal integration within the health system. CHWs administered vaccines in 20 of the 75 countries with documented CHW programs, suggesting the majority of an estimated 3.3 million CHWs globally do not yet administer vaccines. In light of health care workforce shortages and immunization equity gaps, further exacerbated by the COVID-19 pandemic, policymakers should consider task-shifting vaccine administration to CHWs to bolster immunization access for under-reached communities. Additional systematic documentation is needed to further explore best practices to support CHWs as vaccinators, especially related to supply chain, policy, safety, and efficacy.
INTRODUCTION
The Global Vaccine Action Plan aimed to achieve 90% national routine immunization coverage and 80% in every district by 2020.1 While global routine vaccination coverage increased from less than 5% to 86% over the past 4 decades,2 it has stagnated over the last 10 years.3 Between 2010 and 2017, the mortality rate of children aged younger than 5 years decreased by 24%, mainly due to immunization.3 Still, many individuals have insufficient access to routine vaccines, including an estimated 25 million infants each year.4 The COVID-19 pandemic has further heightened inequities by stalling routine immunization services5 as a result of transport disruption, redeployment of the health workforce, and increased risk of COVID-19 at health centers. Routine vaccination coverage decreased from 86% in 2019 to 81% in 2021,4 and the number of children not receiving vaccinations increased to 22.7 million, with 17.1 million not receiving a single dose of diphtheria, tetanus, and pertussis (known as zero-dose children),6 resulting in increased risk of disease outbreaks.
Low- and middle-income countries face severe challenges to immunization coverage, with a persistently large gap in vaccine access compared to high-income countries.5 Access to and availability of vaccines, along with vaccine hesitancy, are the major challenges to increasing vaccination coverage.7,8 Vaccination services rely on health workers to administer them, but a severe health worker shortage in low- and middle-income countries hampers delivery of routine health services, including immunizations.9 To address this shortage, the World Health Organization estimates 18 million more health workers are needed by 2030, primarily in low- and middle-income countries.9
A Role for Community Health Workers as Vaccinators
The Immunization Agenda 2030 identifies universal access to immunization services as an essential component of primary health care10 and aims to reduce the number of zero-dose children by 50% by 2030. The focus of Gavi, the Vaccine Alliance’s 5.0 strategy is to reach zero-dose children,11,12 who live in consistently missed geographic contexts, such as remote rural areas, urban poor communities, and conflict settings.13 They have limited interactions with the public health system and lack the means to access vaccination services.11 Community health workers (CHWs), who often live in and are trusted by under-reached communities, could increase equity in vaccine access for underimmunized and zero-dose children with limited access to health care.
Community health workers could increase equity in vaccine access for underimmunized and zero-dose children with limited access to health care.
Many countries rely on CHWs to improve access to primary health care, especially for hard-to-reach populations.14 CHWs are a cadre of lay health workers who may be paid or volunteer and work in both rural and urban environments.15 The role of CHWs differs notably between countries, but generally, they are considered lay health workers who receive some job training that ranges from several weeks to several years and provide culturally and linguistically appropriate health services to specific communities.16 Some countries have several CHW cadres that may have different scopes of practice or may focus on different sub-populations. Contrary to World Health Organization recommendations,17 CHWs are often considered an informal health cadre and may work with limited preservice training, supervision, competency-based certification, or pay, with some receiving compensation for time or travel in place of a formal salary.16
Decades of research indicate CHWs are trusted agents who help to reduce health disparities by bridging gaps in health care access for underserved communities.15 To promote vaccination, CHWs provide education to families, organize vaccination events, remind parents about childhood immunization schedules, and track immunization rates in their communities.15 CHWs are effective in improving vaccination coverage; however, this is usually through health promotion and health education activities,18–20 rather than by administering vaccines themselves.
In some countries, like Pakistan and Malawi, CHWs also administer vaccines that have been critical to reaching underimmunized and zero-dose communities. CHWs in Pakistan administer the oral polio vaccine (OPV) as well as bacille Calmette-Guerin, measles, and COVID-19 vaccines in some provinces,21,22 while in Malawi, they administer all routine immunizations.23 There are precedents for CHWs administering injections; in at least 20 countries, CHWs administer injectable medication such as contraceptives.24–31
Although much is known about the role of CHWs in improving health system performance, more research is needed to explore opportunities for CHWs to strengthen links between communities and health systems.32 CHWs can play an important role in improving vaccine access by administering vaccines; yet before this review, the literature lacked a comprehensive landscape of countries where CHWs are vaccinating and their circumstances. More systematic documentation is needed to inform policy efforts and deploy CHWs as vaccinators to improve vaccine access and equity.
Our rapid review aims to identify conditions and circumstances under which CHWs can provide vaccination, especially injectables. Specifically, the review attempts to describe where and how CHWs are vaccinating and any potential barriers and facilitators. We did not attempt to identify the efficacy or safety of CHWs as vaccinators.
METHODS
Given the decreasing immunization coverage rates and health workforce shortages, the purpose of this review was to provide timely evidence on the role of CHWs as vaccinators to policymakers and technical partners. Hence, a rapid review was chosen to speed up the systematic review process.33 We asked the following research questions: (1) In which countries are CHWs already administering vaccines? (2) What health systems factors contribute to or detract from the feasibility of CHWs administering vaccines?
Search Strategy and Procedure
The search strategy included peer-reviewed literature, gray literature, and documents supplied by CHW subject matter experts. We included documents published between January 1, 2000 and July 30, 2021 to ensure results addressed recent CHW programs and were applicable to current and future policy. We searched for peer-reviewed literature in PubMed, Cochrane Library (Reviews and Trials), and Web of Science using search terms relating to CHWs, terms relating to vaccination, and terms implying administration of vaccine products. The Box includes a summary of inclusion criteria, and Supplement 1 includes a complete list of search terms, U.S. National Library of Medicine Medical Subject Headings, and Boolean logic as appropriate.
Inclusion Criteria for Rapid Review of Community Health Workers as Vaccinators
Community health workers: As classified by the “Developing and Strengthening Community Health Worker Programs at Scale” reference guide,15 we included documents that referred to community health workers as auxiliary health workers, health extension workers, community health volunteers, lay health workers, or any locally specific term referring to a comparable role.
Study type: Qualitative studies, quantitative studies, evaluations, reviews, mixed methods studies, gray literature
Subject matter: Community health workers administering vaccines
Language: English and French
Date: Published between January 1, 2000 and July 30, 2021
We supplemented the search with gray literature from the following websites and organizations: CHW Central, Community Health Impact Coalition, and Gavi databases. We also reached out to experts in the field of CHW research, policy, and programming to solicit documents for review and conducted reference mining of included documents. These subject matter experts were identified using a snowball approach, first through prior publications and by consulting with individuals from well-recognized organizations such as the Community Health Impact Coalition to request additional connections.
Data Extraction and Analysis
One author screened all titles and abstracts, evaluated documents per the inclusion criteria, and assessed documents for risk of bias using the Joanna Briggs Institute (JBI) critical appraisal tools, a set of tools developed for assessing the quality of published papers.34 For those documents included for which there was no applicable appraisal tool, the reviewer adapted an existing tool for the quality assessment. The following data were extracted into a Microsoft Excel spreadsheet: citation; study type; country; CHW cadre; vaccine administration route and type; and health systems factors related to vaccine administration by CHWs under the following 5 predetermined categories: program history, CHW role, supply chain, gender, and occupational conditions (compensation, supervision, and CHW work environment and experiences). Extracted data related to vaccination administration by CHWs were treated as qualitative data, and extracted content was read and re-read by 1 author. We then conducted deductive content analysis; 1 author coded extracted data and identified subcategories within the 5 predetermined categories.35,36 Coded data and sub-categories were reviewed by all authors and refined in an iterative process through discussion. Once categories were finalized, 1 author generated a table organized by country, cadre name, and category to collate extracted data. We then reviewed this table, and all authors participated in an iterative discussion process to identify key findings for each category.
RESULTS
After the screening process and quality evaluation (PRISMA flow diagram outlined in Figure 137), we retained 32 documents for the review from 497 initial records.21,23,38–67 The review indicated that 23 CHW cadres administered vaccines in 20 countries from 2000 to 2021 (Figure 2). Within the 5 initial health systems categories used to guide data extraction, content analysis revealed additional subcategories (Figure 3). We list vaccinating CHW cadres and related health systems factors in Table 1 and include the full list of documents in Supplement 2.

PRISMA Flow Diagram37 for a Rapid Review of CHWs as Vaccinators
Abbreviations: CHW, community health worker; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.

Countries With Community Health Workers Who Administer Vaccines
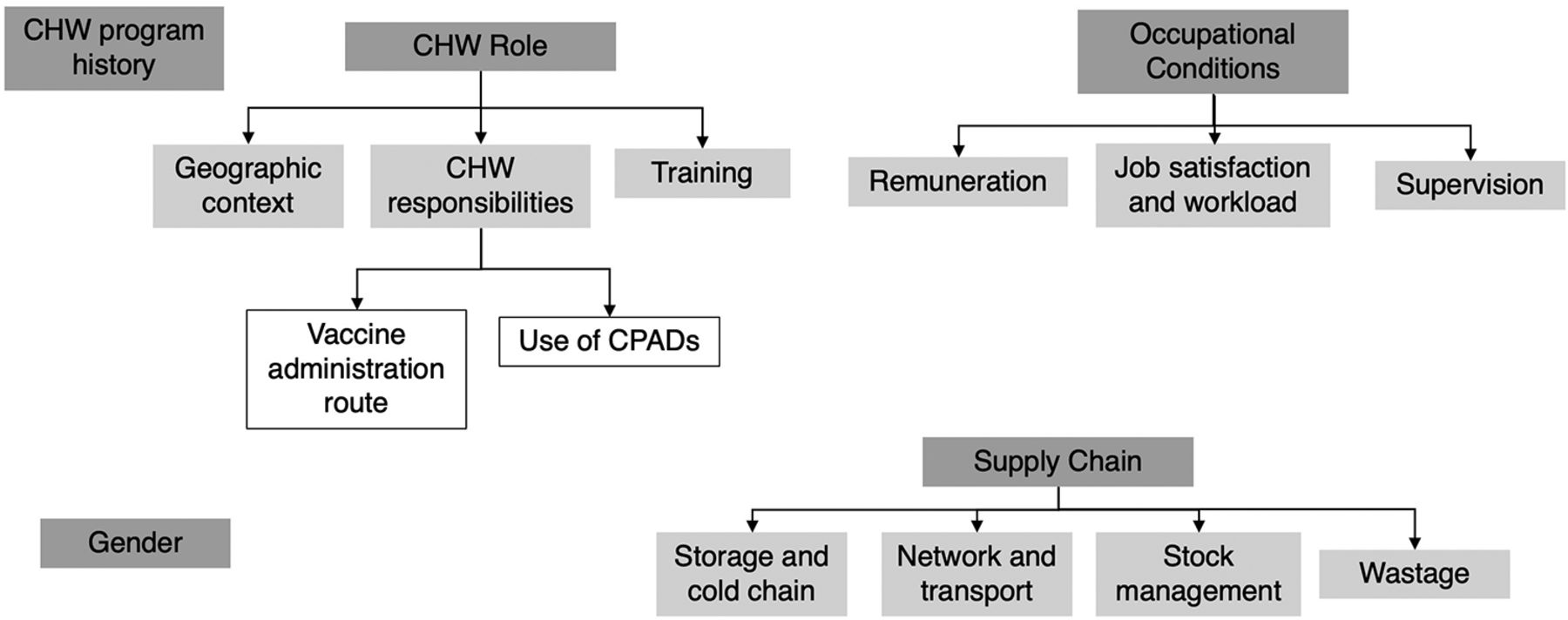
Health Systems Categories Related to CHWs as Vaccinators
Abbreviations: CHW, community health worker; CPAD, compact prefilled auto-disable device.
CHW Cadres That Administered Vaccines and Related Health Systems Factors, by Country
Program History
Many CHW programs gradually increased the scope of work for CHWs over time to include additional tasks, often connected to increasingly formal training, remuneration, and integration into the government public health system.21,23,47,52,58,59,61,63 In 5 countries, CHWs administered vaccines from the earliest days of the national program (Table 2).23,47,59 For other countries, there was no information available on when vaccine administration was added to the CHW scope of work. Overall, we found little discussion of the policymaking process that authorized CHWs to administer vaccines; Pakistan is the only country for which a clear policy process was described.21 Of the 23 CHW cadres identified in the review, 16 cadres administered vaccines as part of an established government program often at a national scale, and 7 cadres were part of a project or temporary campaign (Table 2).
Community Health Worker Vaccine Administration Responsibilities
Many CHW programs gradually increased the scope of work for CHWs over time to include additional tasks.
CHW Role
Geographic Context
In every country identified in this review, the CHW cadres that administered vaccines worked in nonurban contexts (e.g., villages and rural areas).38,39,42,45,47,48,50–53,58–60,63,67 They administered routine immunization at health facilities and in the community, which may involve going door-to-door.38,43,47,50,52–54,58–61,63,65 CHW cadres that administered 1 specific vaccine conducted primarily door-to-door visits.45,48,51,67
CHW Responsibilities
The CHW’s role in many countries focuses on health education and community mobilization. However, the responsibilities of CHW cadres that administered vaccines often included providing other health services, such as first aid or detecting and treating certain medical conditions like TB, malaria, and pneumonia.23,42,45–47,59,63 Fifteen CHW cadres administered all routine immunizations as part of their core responsibilities (Table 2). Eight CHW cadres were trained to administer 1 vaccine as part of a specific vaccination initiative, such as village-based health workers being trained to administer the birth dose of hepatitis B (Table 2).48,67 Five of these 8 cadres only administered vaccines as part of a project or temporary campaign, and from included documents, it was not clear if vaccine administration by CHWs continued after conclusion of the initial project or was established as part of national immunization policy. However, these 8 cadres provide examples of an established CHW cadre’s responsibilities expanding to include vaccine administration, accomplished by introducing 1 specific vaccine to the scope of a CHW cadre that previously did not administer them. In 5 of the 20 countries where CHWs administered vaccines, CHWs also administered injectable contraceptives.21,23,40,50,59,61
Most routine immunizations are delivered via injection, but some are delivered via an oral route. Of the 23 vaccinating cadres identified in this review, 21 cadres administered injectable vaccines, and 2 cadres administered oral vaccines only (Table 2). In Kenya, different CHW cadres have different scopes related to administration route: unpaid community health volunteers administered OPV to rural communities, while paid CHWs administered routine injectable vaccines.46 In the Democratic Republic of the Congo, volunteer vaccinators only administered OPV.49 No information was included about whether the CHW cadres that administered injectable vaccines also administered oral vaccines, except for those in Pakistan. Lady health workers (LHWs) in Pakistan administer injectable vaccines in some provinces, along with OPV.44 Additionally, no information was included on adverse events following immunization related to CHWs administering vaccines.
Many health systems include several cadres of health workers classified as CHWs, and each may have a slightly different clinical scope. For example, one cadre may conduct health assessments and administer medications, while another may conduct community outreach and health education. Eleven countries included in this review had multiple CHW cadres.21,23,39,46,51,59,62,64,66 In 8 of these countries, only 1 CHW cadre administered vaccines.21,23,59,62,64,66 In these cases, the CHW cadre with the highest clinical scope or a role more focused on health care delivery administered vaccines, while other CHW cadres focused on health education, social mobilization, and social support. In India, there is evidence of close collaboration with the other CHW cadres that supported immunization efforts through community mobilization and organizing of vaccination events.39,59,62,64,66
In countries with several cadres of CHWs, the cadre with the highest clinical scope or a role more focused on health care delivery administered vaccines.
In the other 3 countries—Kenya, Indonesia, and Ghana—with multiple CHW cadres, there were 2 CHW cadres that vaccinated.39,45,46,51,59 In these 3 countries, 1 cadre administered routine immunizations, and the other administered 1 specific vaccine during campaigns: tetanus toxoid vaccines to women of reproductive age in Ghana,45 the birth dose of hepatitis B vaccine to newborn infants in Indonesia,51 and OPV as part of supplemental immunization activities in Kenya.39
No CHW cadre focused exclusively on administering immunizations; however, in Malawi and the Democratic Republic of the Congo, the initial concept of the CHW program consisted of a cadre that only administered vaccines.23,59
Use of Compact Prefilled Auto-disable Devices
Administering an injectable vaccine generally requires several steps: (1) acquiring injection materials and maintaining appropriate cold chain requirements for the vaccine vial, (2) reconstituting a vaccine, (3) drawing up the correct dose in a syringe from a multidose vial, (4) administering the injection, and (5) safely disposing of the injection materials.45 Compact prefilled auto-disable devices (CPADs) simplify the injection process by eliminating the need to reconstitute the vaccine and draw the correct dose45,68 and make vaccination easier for health workers who are not accustomed to administering vaccines.45 CPADs cannot be reused, decreasing the risk of bloodborne infection transmission. They can reduce open vial vaccine wastage by eliminating the need to open a multidose vial when only a single dose is required.45,68 Certain CPAD vaccines, such as the hepatitis B Uniject vaccine, are also occasionally stored outside the cold chain,48,51,67 especially when used in conjunction with a vaccine vial monitor, although this is considered off-label use.
CHWs used CPADs to administer vaccines in 6 countries: the birth dose of hepatitis B vaccine in China,48,67 Indonesia,51 and Papua New Guinea,45 and tetanus toxoid vaccines for women of reproductive age in Afghanistan,51 Ghana,45 and Mali.45,51 All 6 CHW cadres who used CPADs did not previously administer immunizations and used CPADs to administer 1 specific vaccine. In Indonesia, after piloting the use of CPADs with community midwives, the government ultimately implemented the program on a national scale. For the other 5 countries where CHWs used CPADs, it was unclear from the included documents if CHWs continued to administer vaccines beyond the initial research or project timelines. There is also evidence of CHWs administering other injectable medications, such as antibiotics and oxytocin, using CPADs.45,68
Training
For CHWs administering routine vaccines, their training ranged from less than a week of formal training for kaders in Indonesia to 2–3 years for community health extension workers in Nigeria.59 There were no data on the training content or if and to what extent training on vaccine administration was included. The only documents that described training specifically for vaccine administration referred to programs that trained CHWs to use CPADs to administer 1 specific vaccine.45,51 These supplemented existing training and ranged from 2 hours to 2 days.45
Occupational Conditions
Remuneration
Remuneration information was available for 18 of the 23 CHW cadres included in the review (Figure 4), of which 13 cadres were salaried employees and received a monthly salary between US$63 per month in Malawi and US$380 per month in Brazil.59 Twelve of these salaried cadres were paid by the government, and 1 was paid by an NGO. Some CHWs also received other forms of compensation or benefits in addition to their monthly salary, such as a uniform, medical equipment, bicycles, per diems, transport reimbursements, paid leave, paid education opportunities, and loans.47,59,63

Remuneration for CHWs Who Administer Vaccines
Abbreviation: CHW, community health worker.
Several CHW cadres—kaders and community midwives in Indonesia,51,59 traditional birth attendants in Ghana and Mali,45 and village health volunteers in Papua New Guinea45—did not receive a salary but may have received stipends or reimbursement for travel expenses and medical treatment, free transportation, food, or accommodation during their training period. Many CHWs, whether salaried or reimbursed, encountered issues with remuneration, such as delayed or missing payments.43,47,58,59
Many CHWs, whether salaried or reimbursed, encounter issues with remuneration such as delayed or missing payments.
Job Satisfaction and Workload
The personal job experiences of CHWs were mentioned for 10 countries included in this review. CHW cadres administering routine immunization described their experience as follows: under-valued, frustrated, overburdened, underpaid, struggled to balance between time at health posts and time in the community, struggled to manage administering immunizations with other responsibilities, lacked a formal career trajectory, and dealt with staffing shortages.23,44,47,52–54,57–59,64
For CHW cadres administering only 1 specific vaccine, some felt their community status was increased through their involvement in a vaccination campaign, and others experienced increased motivation to conduct home visits due to the addition of their vaccination responsibilities.45
Supervision
For 15 of the 20 countries identified in this review (Table 1), documents described some type of direct supervision of CHW cadres that vaccinated. CHW supervision may have included mentoring, evaluation, and on-the-job observation and training related to CHW responsibilities. Supervision may have been conducted at health posts or in the community and may have been provided by a senior CHW with additional supervisory training; a higher-level health worker, such as a nurse, doctor, midwife, or physician’s assistant from a nearby health facility; or a staff person from the local or regional health offices.21,23,40,45,47,53,59,63 For several countries, documents included in the review identified concerns that CHW supervision may be irregular, unpredictable, or insufficient.23,53,59,61
Gender
Globally, the majority of CHWs are female (estimates indicate 70%).69 Specific information about the gender of CHWs was only included for 9 of the 23 CHW cadres included in this review (Table 1). In Ethiopia, India, Indonesia, Pakistan, and Zambia, the CHWs that administered vaccines were mostly women; in some countries, being female was preferred or required for CHW applicants.21,43,44,50,54,59 In Bangladesh and Niger, the CHWs were mostly male,47,59 and in Iran and Papua New Guinea, CHW roles were more evenly split between men and women.45,59,63 There was not enough information in the included documents to indicate patterns in the gender breakdown for CHWs who vaccinated compared to those who did not.
Safety concerns for female CHWs were mentioned for 2 cadres: auxiliary nurse midwives (ANMs) in India and LHWs in Pakistan. ANMs and LHWs, who are all women, have experienced verbal, physical, and sexual abuse while conducting their work in remote areas.43,54,59 In some areas, a male CHW accompanied ANMs when traveling to remote areas in which they did not feel safe traveling alone.62 LHWs may also have been accompanied by their husbands or police escorts while traveling outside their communities, as they may have faced danger or been perceived poorly by outside communities as women traveling alone.43,54,59
Supply Chain
Storage and Cold Chain
CHWs had limited cold chain storage and training.42,55 If they had a refrigerator at their health post, they could store vaccines there; in cases where they did not, they had to transport vaccines in vaccine carriers or cold boxes each time before a session and return any unused vaccine at the end of the day.21,47,59 Some CHWs were not provided with vaccine carriers and made their own arrangements,21 potentially increasing risk to vaccine potency.
In China and Indonesia, CHWs administered hepatitis B vaccines using a CPAD stored outside the cold chain at room temperature,48,51,67 which made vaccine storage and transport for immunization sessions easier. In some cases, CHWs stored unrefrigerated vaccines in their homes in safety boxes, allowing for rapid access when delivering a birth dose of hepatitis B vaccine.51
Network and Transport
Personnel and vaccine supply transportation was also challenging, as many CHWs were located far from facilities where vaccines were stored. CHWs often traveled to pick up vaccines from storage facilities (e.g., health centers) and transported vaccines to the health post or to immunization sessions.21,47,59 To conduct immunization sessions and delivery of other services, many CHWs traveled long distances by foot, bicycle, motorcycle, canoe, and public transportation and may have faced rough, steep terrain.47,49,53,58,62 They may or may not have been given a bicycle, reimbursed for travel costs, or responsible for bicycle repairs.47,53,58
Wastage
Open vial vaccine wastage reflects the portion of a multidose vaccine vial discarded without being administered. Managing open vial wastage could be particularly challenging in rural communities with lower population density where CHWs often work.45,51 The use of CPADs by CHWs could help reduce open vial wastage in remote areas since each device is prefilled with a single dose and prevents the need to use a multidose vial to deliver 1 vaccine.51
Stock Management
CHWs experienced shortages of equipment and medical supplies, such as vaccines, medications, and gloves.47,58,59,61,64 No information was included about the participation of CHWs in vaccine or supply ordering and inventory processes, use of logistics management information systems, reporting of wastage rates, or supply chain supervision.
DISCUSSION
Global Landscape of CHWs Vaccinating
The 23 CHW cadres in 20 countries identified in this review administered vaccines in rural areas where access to immunization services was often limited. As trusted community members trained to both work in a fixed health post and conduct door-to-door visits, CHWs are well positioned to proactively vaccinate underimmunized and zero-dose populations, especially those living in under-reached communities.
This review identified several countries in which CHWs with brief clinical training and experience were taught to vaccinate. These findings suggest it is feasible to task-shift administering vaccines to CHWs with limited experience, provided they receive supplemental training. Many of the vaccinating CHW cadres identified in this review have a broader scope of practice that includes some preventative and curative interventions, as opposed to a role focused on education and community engagement, as is common for many CHW cadres. While task-shifting vaccine administration may be more straightforward for a CHW cadre with a higher clinical scope, this does not appear to be a prerequisite for vaccinating. Use of CPADs, or a similar device, could facilitate expanding the scope of CHWs who do not currently administer vaccines by simplifying vaccine administration and supply chain processes, minimizing opportunities for dosage errors, and reducing wastage related to multidose vials.
Our findings suggest it is feasible to task-shift administering vaccines to CHWs with limited experience provided they receive supplemental training.
Included documents contained limited information on the political process required to add vaccine administration to the scope of work of an existing CHW cadre. Some cadres included in this review administered vaccines as part of a specific project or research experience, but it was unclear if vaccinating remained part of the cadre’s responsibilities or enshrined in national policy after the projects concluded. However, most CHW cadres’ scope of practice changed over time based on ministry of health priorities, and several countries have a CHW cadre to which vaccine administration was added as a responsibility after its initial establishment. This suggests that if ministries of health were to prioritize CHWs administering vaccines, both oral and injectable, then CHWs’ scope could shift to accommodate this if provided adequate training and support. Some governments may be concerned about protection against blame or retaliation in the event of perceived or actual adverse events related to CHWs vaccinating, although this did not come up in the included documents.
Barriers Faced by CHWs Who Vaccinate
Supply Chain
Supply chain barriers faced by CHWs resemble those faced by all health workers delivering services in under-reached communities, especially in rural areas. Supply chains are often designed for cost-efficiency but often do not consider equity to reach the most underserved communities.70 The geographically remote nature of CHWs’ work means they are usually located far from vaccine storage and are often responsible for acquiring vaccines and managing vaccine storage either at their health post or in the community until they are administered. Inadequate cold chain support and training could lead to temperature excursions that can reduce vaccine potency. Vaccines licensed for use in a controlled temperature chain—where certain vaccines are labeled for storage and administration outside the standard cold chain for specific periods of time, under specific conditions—could facilitate CHW vaccine administration, especially in remote areas.71
Managing open vial vaccine wastage is particularly challenging in a rural context with decreased population density, where there may be scenarios in which only 1 dose from a 20-dose vial is needed that day, and the remainder must be discarded. To improve vaccine equity, a vaccine vial should be opened to vaccinate even 1 child. However, high open vial wastage rates are a major issue for immunization programs in low-income countries, as wastage can substantially impact the financial viability of immunization programs.68
Shortages of basic medical supplies and equipment are also a challenge to immunization delivery and CHW safety. Transportation challenges, such as lack of support to reach rural communities and lack of or delayed transportation reimbursement, are also barriers to CHWs administering vaccines.
Occupational Conditions
CHWs also face barriers related to their experience at work, such as being overburdened with tasks, health workforce shortages, and balancing the needs of their health post with time spent in the community conducting immunization. A possible facilitator of CHWs vaccinating could be the existence of 2 or more CHW cadres that can support complementary aspects of immunization. In these situations, 1 cadre focuses on vaccine administration while the other concentrates on education, community engagement, and social mobilization. However, the existence of multiple CHW cadres does not appear to be a necessary precursor to CHWs vaccinating as this was not the case in all countries where CHWs vaccinate.
Vaccinating CHWs also face barriers related to supervision and remuneration. The majority of CHW programs included in this review had a supervision process built into the program that provides support in balancing tasks and acquiring adequate training. However, there are concerns that supervision may be irregular, unpredictable, or insufficient.
Most vaccinating CHW cadres identified in this review are paid government workers, and a small number are unpaid or receive only non-salary compensation such as per diem or transportation reimbursement. However, several vaccinating CHW cadres experience delayed or missing payments despite being salaried. A high proportion of the vaccinating CHW cadres are being paid and exhibited other traits to indicate their integration into the health system in terms of training, supervision, role definition, and financial incentives. Only 14% of CHWs in sub-Saharan Africa receive salaries,72 and comparatively, the vaccinating CHWs represented in this review showed stronger linkages to the government for sustainable, reliable pay and support. As such, while some volunteer cadres do administer vaccines, enshrining sustainable payment mechanisms, ideally by the government, may contribute to the long-term feasibility of vaccination by CHWs.
Enshrining sustainable payment mechanisms, ideally by the government, may contribute to the long-term feasibility of vaccination by CHWs.
Safety concerns are a possible occupational hazard, particularly for female CHWs, and a potential deterrent to participation in immunization activities. These concerns could serve as a barrier to CHWs traveling to conduct immunization activities, which often requires entering the homes of families in remote areas or leaving their communities to participate in campaigns.
Recommendations
We recommend the following to ensure equitable treatment of CHWs who vaccinate and increase immunization access and equity in under-reached and rural communities.
Ensure adequate, reliable remuneration for CHWs. Paying CHWs is considered best practice,17,73 and existing research indicates appropriate financial compensation increases CHW job satisfaction and professional well-being.74,75
Include CHWs in supply chain planning, provide supply chain training, and ensure access to adequate cold chain equipment. In supporting immunization initiatives, especially in rural areas, CHWs who vaccinate manage the final stages of vaccine supply chains. Successful supply chain management is crucial to administer potent vaccines and prevent closed vial vaccine wastage due to temperature excursions.
Ensure reliable access to a dedicated CHW supervisor. Supervision is vital to ensure CHWs have access to necessary training and tools to succeed in their roles. Frequent supportive supervision is an evidence-based strategy for bolstering CHW motivation and improving immunization program quality.76,77
Integrate CHWs as formal health workers in national health systems. Integrating CHWs into national health systems creates an enabling environment for them to be recognized and supported as a professional health cadre and receive certification, standardized pay, training, and professional development opportunities.17,77
Maintain accurate national records of CHW demographic data. Lack of demographic data undermines health system planning and impedes CHWs’ provision of care.76,78 Increased availability of demographic data for CHWs could improve governments’ ability to train, pay, and provide other professional support for CHWs to successfully vaccinate.
We also recommend additional research to conduct a deeper landscape of countries in which CHWs administer vaccines. Partnering with country experts for this landscaping process would be crucial as this review identified a lack of current documentation on whether CHWs are vaccinating, and much of the data included in this review did not come from published literature. Finally, to further understand the needs of and provide adequate support for CHWs who vaccinate, additional research into acceptability of CHWs as vaccinators, necessary supply chain training and support, and the safety and efficacy of CHWs administering vaccines is needed.
Limitations
This review serves as a first step in expanding and synthesizing available research to provide a global landscape of where and how CHWs are administering vaccines. One key limitation was the scarcity of information available on CHWs vaccinating, and for several CHW cadres only 1 source was available. We included 5 documents despite some quality concerns; these articles were retained to gather information from relevant descriptive sections even if the analytical content was not of the highest quality. Additionally, few of the included documents are specifically focused on the role of CHWs administering vaccines. As CHWs are often considered an informal cadre, their work is not always systematically documented, so there may be countries in which CHWs are vaccinating that were not captured in this review.
Furthermore, this review identified a lack of information on the ways CHWs interface with key aspects of the vaccine supply chain. This is concerning given that supply chain is such an important factor in immunization delivery, regardless of who is administering the vaccine. Potent vaccines need to be available when and where they are needed by communities. There was also limited information regarding the political processes and policy guidelines required to legally allow CHWs to vaccinate. Due to limited availability of demographic data in the included documents, there is no indication that gender-related factors are either a barrier or a facilitator to CHWs vaccinating. The lack of demographic data for CHWs is a widespread issue across countries due to poor data management and inaccurate or frequently unavailable data on the number and location of active CHWs.78
Finally, clearly defining CHWs is challenging due to the diversity of definitions between countries. This review considered several cadres as CHWs that some may consider better categorized as a more advanced health worker cadre due to their higher-level training requirements and scope of work.
CONCLUSIONS
The review identified 23 CHW cadres that vaccinated in 20 countries. These vaccinating CHW cadres support equity in immunization access for rural and under-reached communities. CHWs who vaccinate face the following challenges: (1) inadequate supply chain training, (2) inadequate cold chain equipment, (3) transportation for supplies and to communities, (4) heavy existing workload, (5) inadequate or irregular remuneration, (6) inadequate or irregular supervision. To improve immunization coverage in underimmunized and zero-dose communities, countries where CHWs vaccinate should provide CHWs with adequate remuneration, supervision, supply chain support and management, and formal integration within the health system.
CHWs administered vaccines in 20 of the 75 countries with documented CHW programs, suggesting the majority of an estimated 3.3 million CHWs globally do not yet administer vaccines.78,79 In light of health care workforce shortages and immunization equity gaps, further exacerbated by the COVID-19 pandemic, there may be settings where task-shifting vaccine administration to CHWs should be considered to bolster immunization access for under-reached communities. To further explore best practices to support CHWs as vaccinators and encourage task-shifting in those countries where CHWs do not currently vaccinate, additional systematic documentation is needed, especially related to supply chain, policy, safety, and efficacy.
Acknowledgments
The authors thank the following individuals who supported this review: Stephen Hodgins, Hope Ngwira, Nicholas Leydon, Dr. Mrunal Shetye, Melissa West, and Carey Carpenter Westgate.
Funding
This work was supported by Gavi, the Vaccine Alliance. Gavi did not play any role in the research design, execution, analysis, interpretation, or reporting.
Author contributions
EG made substantial contributions to the conception and design of the work; the acquisition, analysis, and interpretation of data for the work; and drafting and critically revising the article. MZ, RA, and LMK made substantial contributions to the conception and design of the work, interpretation of data for the work, and drafting and critically revising the article. All authors provided final approval of the version to be submitted and agree to be accountable for all aspects of the work.
Competing interests
None declared.
Notes
Peer Reviewed
First published online: February 14, 2023.
Cite this article as: Gibson E, Zameer M, Alban R, et al. Community health workers as vaccinators: a rapid review of the global landscape, 2000–2021. Glob Health Sci Pract. 2023;11(1):e2200307. https://doi.org/10.9745/GHSP-D-22-00307
- Received: June 30, 2022.
- Accepted: January 10, 2023.
- Published: February 28, 2023.
- © Gibson et al.
This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visit https://creativecommons.org/licenses/by/4.0/. When linking to this article, please use the following permanent link: https://doi.org/10.9745/GHSP-D-22-00307
REFERENCES









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Statistics from Altmetric.com
Jump to section
Related Articles
Cited By...
- No citing articles found.