


INTRODUCTION
In the past decade, the field of family planning has seen an acceleration in conversations about self-care interventions and, within that, a resurgence of discussions on reproductive empowerment. The World Health Organization (WHO) defines self-care as1:
the ability of individuals, families, and communities to promote health, prevent disease, maintain health, and cope with illness and disability with or without the support of the health provider.
Self-care spans a range of practices including self-awareness, self-testing, and self-management, and self-care interventions are tools that support self-care.1 Reproductive empowerment is defined as the capacity of individuals to achieve their reproductive goals,2 and it is recognized as a fundamental principle for self-care.
Understanding the relationship between self-care and empowerment is necessary to improve the design, implementation, and scale-up of family planning self-care interventions. Yet, evidence on the relationship between reproductive empowerment and self-care, including the strength of the association, the direction of the association, or the hypothetical causality, is inadequate. A recent systematic review we conducted to understand the relationship between contraceptive self-care interventions and reproductive empowerment found clear gaps in the gray and published literature.3 Following the WHO guideline on self-care interventions,1 certain user-dependent methods were always included (e.g., oral contraceptive pills, condoms, rhythm method), whereas other interventions were included in certain circumstances (e.g., contraceptive injectables when self-injected, fertility awareness tools including digital apps, urine pregnancy tests when used for initiating a family planning method). Client-facing digital technologies were included if they (1) were accessible by clients with or without a health care provider; and (2) were created to provide individualized information, guidance, or self-management of contraception to enhance access, acceptability, use of and/or intention to use contraception. The vast majority of the existing evidence was for condoms, most of the research had been conducted in high-income countries, and analyses provided minimal evidence on the relationship, in any direction, between self-care and reproductive empowerment. Furthermore, even though measures exist to assess reproductive empowerment-related concepts, including scales validated in Kenya, Nigeria, Zambia, Ethiopia, Uganda, and the United States, these were not used in the studies eligible for inclusion in the review.4–9
Understanding the relationship between self-care and empowerment is necessary to improve the design, implementation, and scale-up of family planning self-care interventions.
Scales are11,12:
measurement instruments that are collections of items combined into a composite score … intended to reveal levels of theoretical variables not readily observable by direct means.
Family planning programmers and researchers are often interested in measuring constructs such as attitudes, self-efficacy, or empowerment that are not directly observable to determine if their program objectives are being met or why there might be gaps in meeting their objectives. Further, using the same scale to measure a construct across populations, geographies, and/or contexts fosters comparability and produces generalizable knowledge about that construct. The goal of this commentary is to garner support from the family planning community to use existing, validated reproductive empowerment scales to generate comparable evidence and answer questions such as, “Are family planning self-care interventions empowering?” and, “Are self-care interventions more readily used by those who feel more empowered?” Here, we summarize the scales and the results of our thematic analysis to help programmers and researchers select the most appropriate scales to inform their family planning self-care programming.
THE FRAMING OF REPRODUCTIVE EMPOWERMENT
A place to start understanding reproductive empowerment is by defining empowerment itself. Kabeer suggested a definition of empowerment that is commonly used12:
the expansion in people's ability to make strategic life choices in a context where this ability was previously denied to them.
According to Kabeer, the core conditions of empowerment are agency, resources, and achievement.11 Reproductive empowerment is a type of empowerment that is specific to the life domain of reproduction, including contraception; other types of empowerment in different life domains include economic, legal, and social.
Several frameworks related to reproductive health and empowerment have been developed, and they focus on dimensions such as individual and structural power dynamics, as well as psychosocial processes, beginning with the existence of choice and progressing to the exercise and achievement of choice.8,13–17 Despite these variations, reproductive empowerment is generally conceptualized as the result of the interaction between individual and structural factors.12 For the systematic review on reproductive empowerment and contraceptive self-care, we used the Reproductive Empowerment Framework developed by the International Center for Research on Women (ICRW) with funding from the U.S. Agency for International Development and in partnership with MEASURE Evaluation.2 The ICRW framework adopts Kabeer's conditions of agency and resources as its own core components.
Reproductive empowerment is generally conceptualized as the result of the interaction between individual and structural factors.
Agency, at the center of the ICRW's Reproductive Empowerment Framework, is defined as individuals' capacity to take deliberate actions to achieve their reproductive goals. The framework describes 3 levels of agency: individual, immediate relational, and distant relational. Individual agency includes comprehensive knowledge, physical and mental health, self-efficacy, and critical consciousness. Immediate relational agency includes characteristics of relationships such as emotional intimacy, communication quality, respect for bodily integrity, and social support. And thirdly, distant relational agency includes resources such as the political, legal, and policy environments, health system culture; gender and reproductive norms; and the physical, cultural, and economic environments. In this framework, self-efficacy is considered a “resource” for empowerment.
According to ICRW,2
Resources are “enabling factors” that may act as catalysts for empowerment within the context of specific relationships.
Agency and self-efficacy are integral components to those interested in measuring and increasing reproductive empowerment in programs and research.
Reproductive autonomy, another construct of interest to those considering reproductive empowerment, has been defined by Upadhyay et al. as4:
having the power to decide about and control matters associated with contraceptive use, pregnancy, and childbearing.
The authors further note that “reproductive autonomy is one domain within the overarching construct of women's empowerment,” which is defined as “the expansion in women's ability to make strategic life choices where this ability was previously denied them,” citing the Kabeer definition. With this framing of reproductive empowerment in mind, we searched for measures that aligned with this framing and the conditions of agency, resources, and autonomy.
MAPPING MEASURES OF REPRODUCTIVE EMPOWERMENT
We searched the peer-reviewed literature to identify existing scales that measure reproductive empowerment and understand how reproductive empowerment is conceptualized within those scales. We examined references of the articles from the systematic review previously mentioned and searched for related articles using PubMed and Google Scholar. This was not a systematic literature review. We identified 5 validated scales related to reproductive empowerment that may be of interest to family planning programs (Table)5–10,18: The Reproductive Autonomy Scale, the Reproductive Empowerment Scale, the Contraceptive Self-Efficacy among women in sub-Saharan Africa (CSESSA) scale, Women's and Girls' Empowerment in Sexual and Reproductive Health (WGE-SRH) index, and Sexual and Reproductive Empowerment Scale for Adolescents and Young Adults. The first 4 scales focus on women of reproductive age, and the last scale focuses on youth (aged 15–24 years) of both genders.
Landscape of Validated Scales for Reproductive Empowerment
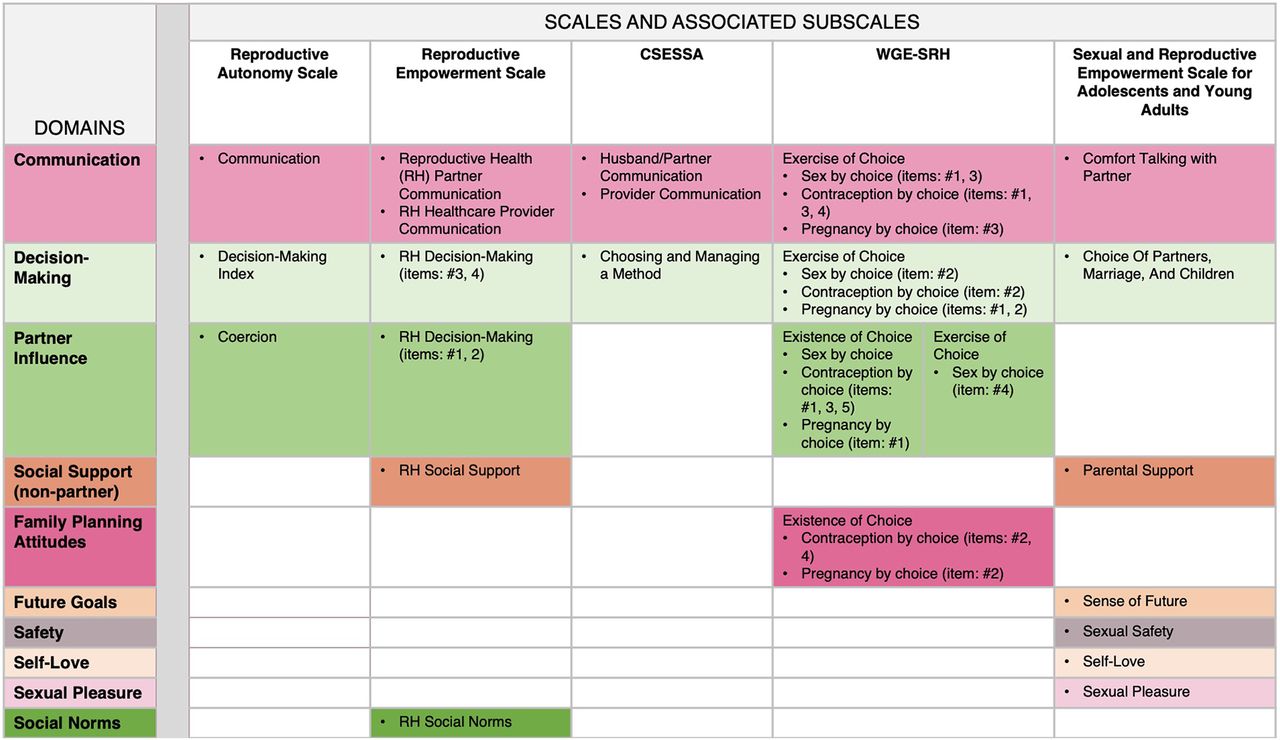
After examining the existing reproductive empowerment-related scales, we observed thematic similarities across the scales' items even though the authors of the scales used different labels for their constructs. For example, some scales may label an item as “choice” while another scale may label a similar item as “communication.” Programs that seek to identify activities to increase their clients' reproductive empowerment and measure change in reproductive empowerment after implementing these activities may face inconsistencies in terms and definitions. This led us to create a map by thematically grouping the items within the 5 reproductive empowerment-related scales into domains that could be the focus of reproductive empowerment activities within family planning programs (Figure 1).
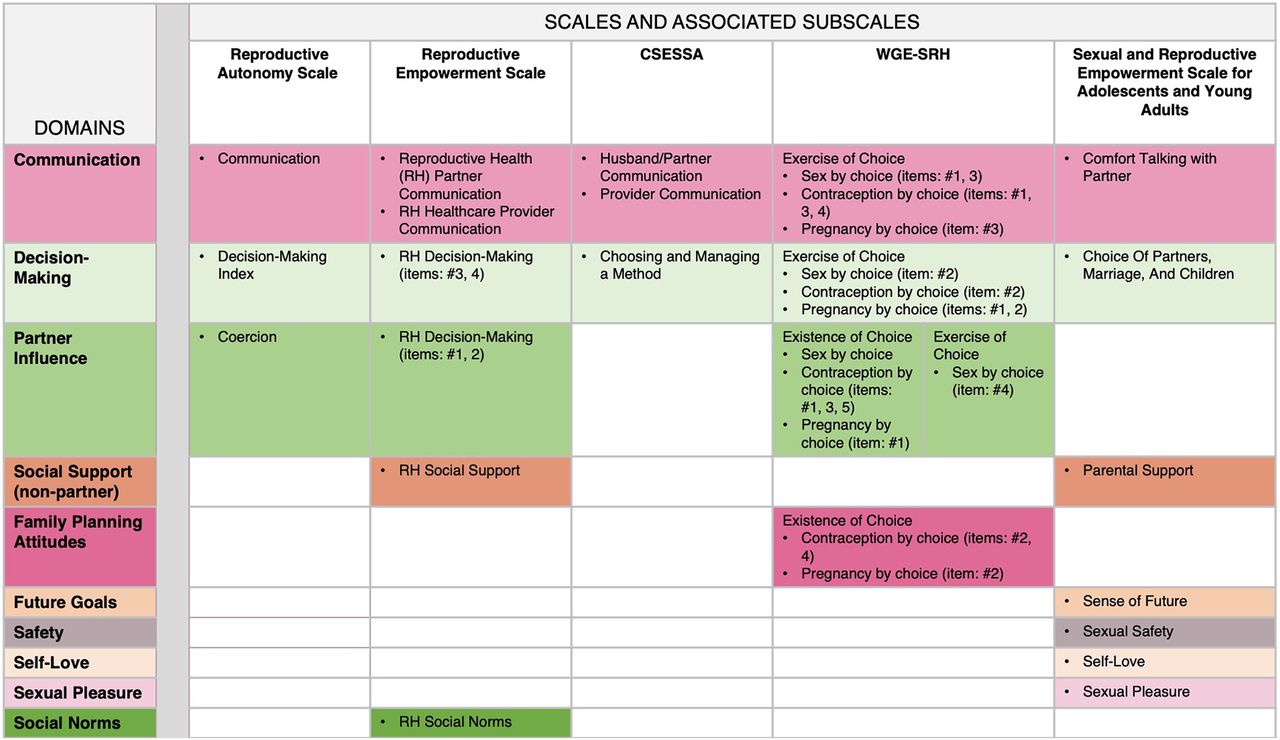
Map of Validated Reproductive Empowerment Scales by Domain
Abbreviations: CSESSA, Contraceptive Self-Efficacy among women in sub-Saharan Africa; RH, reproductive health; WGE-SRH, Women's and Girls' Empowerment in Sexual and Reproductive Health.
We mapped the items in the existing reproductive empowerment scales by theme into 10 domains.
We first mapped the domains using the scale authors' labels (not shown). This resulted in 10 domains: (1) communication; (2) decision making; (3) choice (of method, of management of method, and of partner); (4) coercion; (5) social support; (6) future goals; (7) safety; (8) self-love; (9) sexual pleasure; and (10) social norms.
Next, we reviewed the content of the items within each domain (as described by the scale authors) to identify similarities or differences between the items. We also considered whether the current labels reflected the content of the items when looking across the scales. We observed that 3 of the scales had items that measured the influence of sexual partners, and therefore, we grouped the items into a “partner influence” domain. This new domain included the items from the coercion subscale of the Reproductive Autonomy Scale, items #1 and #2 from the RH decision-making subscale of the Reproductive Empowerment Scale, and all 4 items under WGE-SRH's existence of choice, sex by choice subscale, as well as contraception by choice items #1, #3, and #5, pregnancy by choice item #1, and exercise of choice, sex by choice item #4. When we looked at the items scale authors put under the “choice” domain, we noticed they were heterogeneous. We redistributed these items thematically into the existing decision-making and communication domains and the new partner influence domain. Specifically, for the WGE-SRH under exercise of choice, sex by choice item #2, contraception by choice item #2, and pregnancy by choice items #1 and #2 mapped onto the decision-making domain. Also, CSESSA's choosing and managing a method subscale and the Adolescent and Young Adults scale's choice of partners, marriage, and children mapped on the decision-making domain. Several WGE-SRH items under exercise of choice mapped onto the communication domain: sex by choice items #1 and #3; contraception by choice items #1, #3, and #4; and pregnancy by choice item #3. There were a few items from the WGE-SRH (contraception by choice items #2 and #4 and pregnancy by choice item #2) that did not fit in other domains, and we grouped these under a new domain called “Family planning attitudes.” Thus, we ended the thematic process with the following 10 domains and definitions.
Communication: Any item indicating an exchange of thoughts, words, or ideas either verbally or nonverbally by the interviewee to another person or to a group of people
Decision making: Any item referring to a potential choice being made by the interviewee about their childbearing; sex; marriage; family planning method use, type, and management; pregnancy; child-rearing; and abortion
Partner influence: Any item indicating coercion or consequences by an interviewee's sexual partner over family planning method use, pregnancy, and sex
Social support: Any item indicating help given to an interviewee by family, friends, or other people in their community (excluding the interviewee's sexual partner)
Family planning attitudes: Any item indicating a personal gain or worry due to the use of family planning methods or spacing between pregnancies
Future goals: Any item indicating short-term or long-term plans for the interviewee
Safety: Any item indicating the interviewee feeling free of harm
Self-love: Any item indicating confidence, self-worth, and ownership of oneself
Sexual pleasure: Any item indicating feelings of enjoyment or fulfillment for the interviewee or their partner(s)
Social norms: Any item indicating societal values experienced by the interviewee through friends or family
Looking across the scales in our map, we notice that items within the communication domain (Figure 2) and decision-making domain (Figure 3) are represented in all 5 scales and that items from the partner influence domain (Figure 4) are found in 3 of the scales. Items measuring social support (from non-partners) are found in 2 scales, and the rest of the domains are found in only 1 scale. Similar to our findings, a recent systematic review investigating the measurement properties of women empowerment scales in sexual and reproductive health found the most common domains explored were decision making, freedom of coercion, and communication with a partner.19

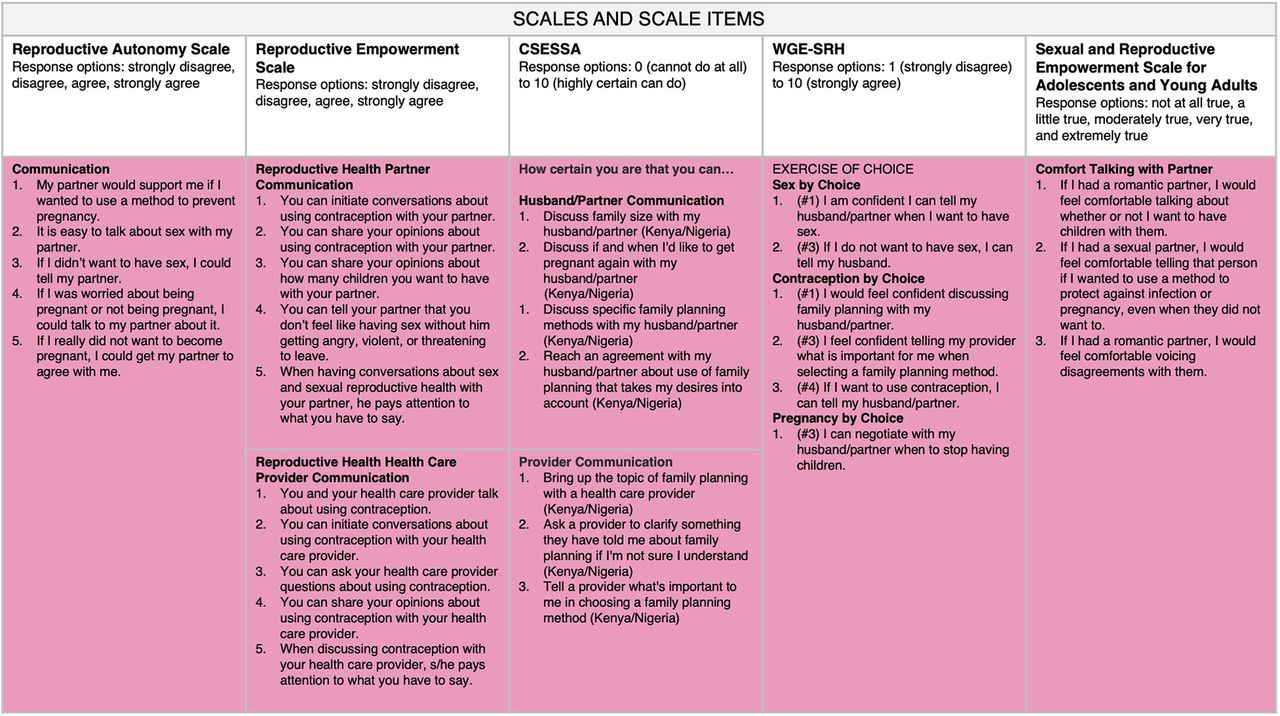
Reproductive Empowerment Scales and Scale Items Within the Communication Domain
Abbreviations: CSESSA, Contraceptive Self-Efficacy among women in sub-Saharan Africa; WGE-SRH, Women's and Girls' Empowerment in Sexual and Reproductive Health.

Reproductive Empowerment Scales and Scale Items Within the Decision-Making Domain
Abbreviations: CSESSA, Contraceptive Self-Efficacy among women in sub-Saharan Africa; RH, reproductive health; WGE-SRH, Women's and Girls' Empowerment in Sexual and Reproductive Health.
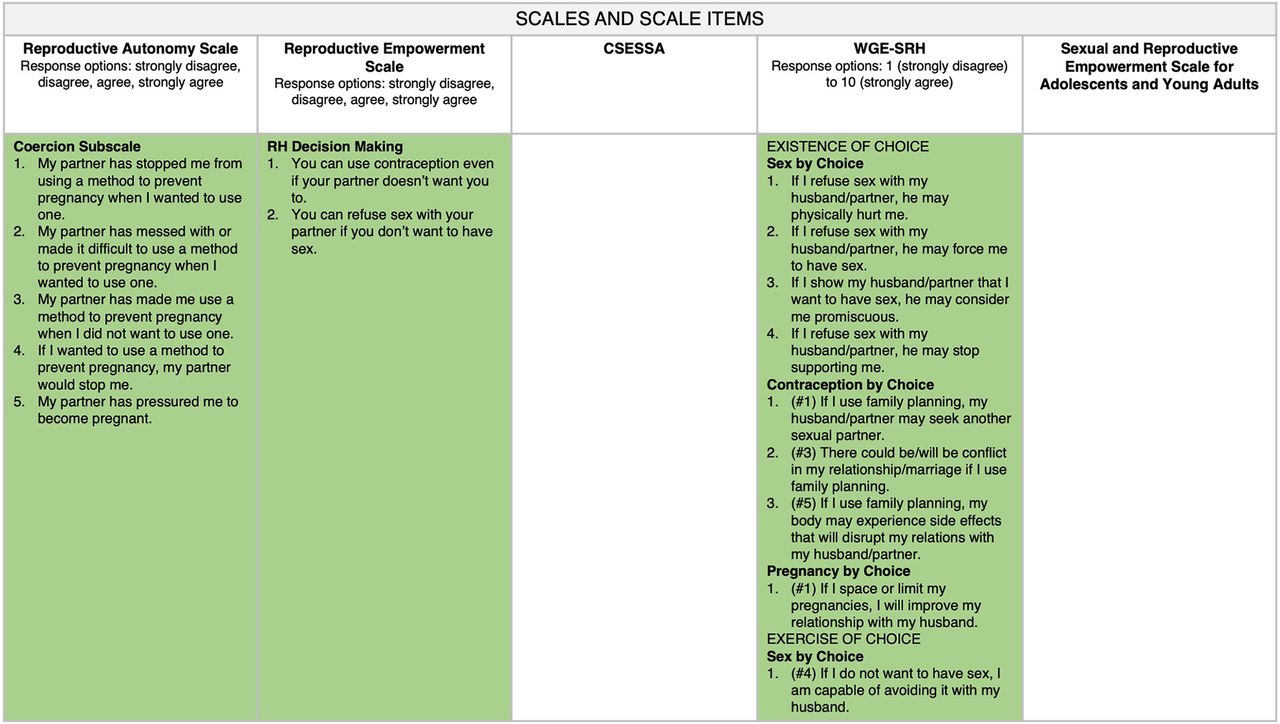
Reproductive Empowerment Scales and Scale Items Within the Partner Influence Domain
Abbreviations: CSESSA, Contraceptive Self-Efficacy among women in sub-Saharan Africa; RH, reproductive health; WGE-SRH, Women's and Girls' Empowerment in Sexual and Reproductive Health.
HOW TO USE THE MAP
Depending on which construct(s) of reproductive empowerment family planning programmers and researchers want to focus on, they may use our map (Figure 1) to identify the scale(s) and/or scale items to measure those specific constructs. The choice of which scales to use should be driven by a context-relevant, clear theory of change. This map serves as a tool to help narrow down the scales based on the program's theory of change. For example, a program or study may be interested in measuring women's agency because they want to determine if self-injectable contraceptive use is empowering. In this situation, they may want to consider using the Reproductive Empowerment Scale because it meets the 3 levels of agency outlined by the Reproductive Empowerment Framework through its 5 domains: individual (partner influence and decision making), immediate relational (communication), and distant relational (social support and social norms) agency. Programs or studies interested in measuring women's contraceptive self-efficacy may want to use the CSESSA because it measures respondents' confidence in performing specific behaviors related to initiating, managing, and continuing use of contraception. However, if items measuring communication are already covered in your questionnaire by another scale, perhaps consider only using the CSESSA subscale “choosing and managing a method” to avoid redundancy and decrease respondent burden. Those interested in measuring autonomy may want to consider using the Reproductive Autonomy Scale or WGE-SRH because of these scales' broad coverage of the topic with the domains of partner influence, communication, and decision making. Finally, the Sexual and Reproductive Empowerment Scale for Adolescents and Young Adults may be useful for programs wanting to measure reproductive autonomy among adolescents.
Family planning programmers and researchers may use the map to identify the scales and/or items to measure specific constructs of reproductive empowerment.
CONCLUSION
Reproductive empowerment is a broad concept. When measuring reproductive empowerment, there are many existing frameworks, definitions, and scales to draw from. We recommend consistently using existing scales rather than creating new measures or items and measuring specific reproductive empowerment domains. This will allow us to collectively build the evidence base on reproductive empowerment in a way that will advance family planning self-care programming by providing comparable evidence. We mapped the domains and items measured by 5 existing scales. Communication, decision making, and partner-influence are the most measured domains among the scales we examined; however, measures of other reproductive empowerment domains are available and may be of interest to programs depending on their context and focus. Our analysis and mapping may be a useful resource for family planning self-care programmers or researchers, as well as those working in reproductive health in general, who want to focus on certain construct(s) within the broader reproductive empowerment framework.
Acknowledgments
The authors are grateful to Aurélie Brunie, Kate Murray, and Kathleen Ridgeway for their helpful review of the manuscript.
Funding
Support for this research was made possible by the American People through the United States Agency for International Development (USAID). Research for Scalable Solutions (R4S) is a global project funded by USAID and led by FHI 360 in partnership with Evidence for Sustainable Human Development Systems in Africa, Makerere University School of Public Health in Uganda, Population Services International, and Save the Children. The information provided does not necessarily reflect the views of USAID or the United States Government.
Author contributions
HMB conceived the analysis. HMB and RT conducted the analysis and wrote the first draft of the commentary.
Competing interests
None declared.
Notes
Peer Reviewed
First published online: June 17, 2022.
Cite this article as: Burke HM, Thomas R. Thematic analysis and mapping of reproductive empowerment scales: a tool for family planning self-care programming and research. Glob Health Sci Pract. 2022;10(3):e2100794. https://doi.org/10.9745/GHSP-D-21-00794
- Received: December 8, 2021.
- Accepted: May 11, 2022.
- Published: June 29, 2022.
- © Burke and Thomas.
This is an open-access article distributed under the terms of the Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in anymedium, provided the original author and source are properly cited. To view a copy of the license, visit https://creativecommons.org/licenses/by/4.0/. When linking to this article, please use the following permanent link: https://doi.org/10.9745/GHSP-D-21-00794









{kind=link}
{kind=link}
{kind=link}
{kind=link}
Statistics from Altmetric.com
Jump to section
Related Articles
Cited By...
- No citing articles found.